




FREE Complications Webinar
Want to overcome your fear of complications and confidently master anatomy?
Join us for one of Dr Tim's FREE upcoming webinars.
Check dates here and save your spot
 Dr Tim Pearce
Dr Tim Pearce
A few years ago, a colleague experienced their first vascular occlusion while injecting the philtrum. They handled the situation well, managing it over a hard weekend with multiple visits and treatments and a full 48 hours devoted to resolving the problem for their patient. But afterwards, they were left with a terrible sense of fear about restarting. They emailed asking the question that sits in the back of every injector’s mind after a complication: how can I ever avoid this happening again?
That fear is understandable, and it does not have to be paralysing. The anatomy of the philtrum creates specific risks that, once you understand them properly, you can take practical steps to manage. The columella artery is the vessel at the centre of this conversation, and getting comfortable with its course and behaviour is what separates injectors who treat with confidence from those who avoid the area altogether.
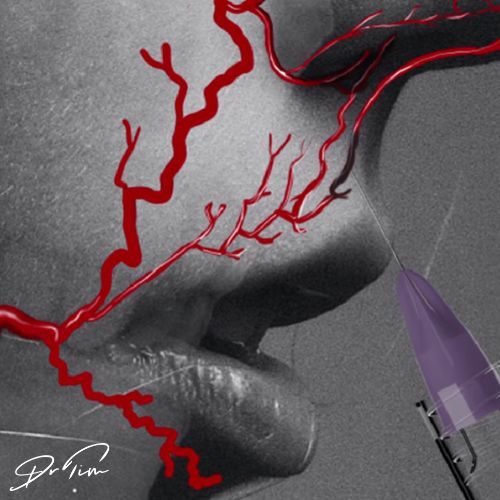
The columella artery, when viewed from the front, often runs parallel to and even within the philtral columns. It branches from the superior labial artery, which we know sits most commonly underneath the orbicularis oris muscle, though it can also run within the muscle and occasionally superficial to it.
According to cadaveric studies, the columella artery has two branches: a deep branch and a superficial branch. The deep branch contributes blood supply to the nasal septum, which carries its own clinical significance because a vascular occlusion in the lip could potentially affect this area too. The superficial branch naturally becomes superior to the orbicularis oris muscle, which makes it more vulnerable to the needle during philtrum treatment.
This is where the anatomy of the philtrum itself creates the problem. The philtrum curves, and the nasolabial angle means the artery must make its way into the path of a straight needle pointed towards the nose. The deeper your needle travels, the closer it gets to the columella artery. This relationship between needle depth and arterial proximity is the single most important concept to grasp when treating this area.
The shape of the philtrum works against you in a way that other injection sites do not. A straight needle inserted into a curved structure will naturally change its depth as it progresses, and this tendency for the needle to travel deeper into the muscle as it follows the curve of the philtrum catches injectors out. You might start at a safe depth and gradually end up much closer to the columella artery than you intended, without any conscious change in your technique.
This is compounded by the fact that the needle runs parallel to the artery in this area. In most injection sites, you might cross an artery briefly as your needle passes through, and the risk exists at a single point. When the needle and the artery are running in the same direction, the window of risk extends along the entire length of your injection. If you are performing a linear thread technique through the philtrum, the needle could be tracking alongside or even within the vessel for several millimetres.
There are several things you can do to become safer when treating the philtrum, and none of them require you to avoid the area entirely.
Limiting your treatment to the lower two thirds of the philtrum is one of the most straightforward adjustments you can make. The more superior your injection, the closer the artery becomes, so staying in the lower portion of the philtrum gives you a larger margin of safety. This is a simple geographic boundary that reduces risk without compromising the treatment outcome for most patients.
Being conscious of your needle depth matters enormously here. Because the philtrum curves and the needle does not, the tip naturally drifts deeper as you advance. One practical technique to manage this is pinching the philtrum into a straighter shape before you inject, which aligns the tissue more closely with the shape of the needle and helps maintain a consistent depth throughout the thread. This physical manipulation of the tissue is something you can practise and develop a feel for over time.
Positive aspirations are actually quite common at the top of the philtrum in aesthetic practice, and there is no clinical need to go as deep as many injectors do in most patients. Staying superficial where you can is a meaningful risk reduction strategy.
Because the needle runs parallel to the artery in this area, a single aspiration at the start of a linear thread only tells you about one point along that track. You could aspirate negative at the beginning and then move directly into the vessel as you advance. This is where increasing the number of aspirations during a single pass becomes valuable.
When performing a linear thread through the philtrum, you can aspirate as many times as you like. Two or three aspirations along the length of the thread would significantly increase the sensitivity of the technique in terms of detecting whether you are in an artery. Each negative aspirate is decreasing the probability of being intraarterially prior to injecting. Mathematically, the cumulative effect of multiple negative results gives you substantially more confidence than a single test.
The technique takes almost no additional time once you are used to it, and it causes no harm. The benefits outweigh any drawbacks quite clearly. For injectors who have been taught that a single aspiration is sufficient, adding two or three more along a philtrum thread is an easy upgrade that requires no new equipment, no additional training, and no change to your overall treatment plan.
If you do suspect a vascular occlusion during or after a philtrum treatment, the anatomy should guide your assessment. The columella artery’s course means you need to check more than just the injection site. Examine the philtrum itself, then the columella, the nose tip, and inside the nostrils towards the septum. That deep branch supplying the nasal septum means an occlusion originating in the lip could show signs in areas your patient might not immediately connect to their lip treatment.
Get a cotton bud and test capillary refill in each of these areas carefully. The speed at which colour returns after you press and release the tissue tells you whether blood flow is intact. Checking each area systematically, rather than focusing only on where you injected, gives you the fullest picture of what is happening and whether you need to escalate your management.
The colleague who emailed after their first occlusion was experiencing something very common among aesthetic injectors. A complication, even one that resolves well, can shake your confidence in a way that makes you question whether you should be treating certain areas at all. The answer lies in understanding the anatomy well enough that you know precisely why the complication occurred and what you can change to reduce the probability of it happening again.
Limiting depth, treating the lower philtrum, pinching the tissue to match the needle, and aspirating multiple times along a linear thread are all concrete adjustments that meaningfully reduce risk. They are not guarantees, because no technique eliminates risk entirely, but they represent a thoughtful approach grounded in anatomical understanding that allows you to treat with appropriate confidence.
The philtrum is a valuable treatment area that patients want addressed. Walking away from it entirely because of fear means your patients miss out on a treatment that can beautifully enhance the lip and cupid’s bow. Walking into it armed with better knowledge of the columella artery, a refined technique, and a systematic approach to detecting problems early is a much better position to be in.
Join us for one of Dr Tim's FREE upcoming webinars.
Check dates here and save your spot

Dr Tim Pearce MBChB BSc (Hons) MRCGP founded his eLearning concept in 2016 in order to provide readily accessible BOTOX® and dermal filler online courses for fellow Medical Aesthetics practitioners. His objective was to raise standards within the industry – a principle which remains just as relevant today.
Our exclusive video-led courses are designed to build confidence, knowledge and technique at every stage, working from foundation level to advanced treatments and management of complications.
Thousands of delegates have benefited from the courses and we’re highly rated on Trustpilot. For more information or to discuss which course is right for you, please get in touch with our friendly team.





