




FREE Complications Webinar
Want to overcome your fear of complications and confidently master anatomy?
Join us for one of Dr Tim's FREE upcoming webinars.
Check dates here and save your spot
 Dr Tim Pearce
Dr Tim Pearce
The frontalis muscle is probably the hardest area to treat when you first start injecting, and the reason so many injectors struggle with it in their first 18 months comes down to a combination of wildly variable anatomy between patients and the fact that we are always trying to only partially treat it, which means there is always some movement left over and getting the balance right takes real clinical judgment that no single injection pattern can replace.
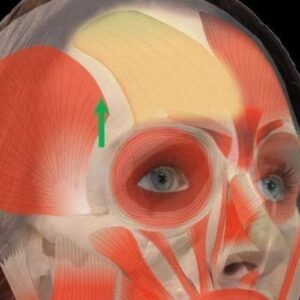 The differences between patients are far more dramatic than most training courses prepare you for, with some people presenting with small foreheads and others with long foreheads, muscles that look like two separate plates versus muscles that appear as one continuous plate, and in men the frontalis muscle often extending well beyond the hairline or where the hairline once sat before it receded. These anatomical differences matter because the aesthetic goals are also different between patients, and a feminine arch that looks elegant on a female patient can look sinister or odd on a male patient, which means you need to learn a set of principles that allow you to treat any forehead rather than memorising a simple injection pattern that someone tells you to apply universally.
The differences between patients are far more dramatic than most training courses prepare you for, with some people presenting with small foreheads and others with long foreheads, muscles that look like two separate plates versus muscles that appear as one continuous plate, and in men the frontalis muscle often extending well beyond the hairline or where the hairline once sat before it receded. These anatomical differences matter because the aesthetic goals are also different between patients, and a feminine arch that looks elegant on a female patient can look sinister or odd on a male patient, which means you need to learn a set of principles that allow you to treat any forehead rather than memorising a simple injection pattern that someone tells you to apply universally.
The side effects that come from the frontalis are almost all traceable to using a blanket approach, either too much toxin on every patient or the same injection pattern on everyone you meet. Over-treating the middle creates a medial brow ptosis with a lateral brow lift, producing the characteristic spock brow that patients find so distressing. Over-treating laterally can flatten the eyebrow arch and leave movement in the middle, creating a sad appearance. Over-treating the whole muscle leaves the patient looking tired as the eyebrows settle, and in patients whose skin rolls straight from the forehead onto the eyelids it can even mimic bilateral eyelid ptosis.
The most practical starting point for any frontalis treatment is to map out where you are not going to inject before deciding where you will, because by the time you have identified the safety margin of approximately two centimetres from the orbital rim to prevent brow ptosis and marked any areas of aponeurosis where there is no muscle and toxin would simply be wasted, the remaining treatment area is usually quite small and the decisions become much more manageable.
First treatments with a new patient should be approached as a staged process where you make your best clinical judgment but deliberately leave room for a top-up at a follow-up appointment, because if you try to achieve the perfect result in a single session you are more likely to cause an over-treatment such as loss of eyebrow arch or a brow ptosis, and at that point your options for correction are far more limited than they would have been if you had simply planned to refine the result in stages. After two or three treatment cycles with the same patient you will know exactly where to inject and the follow-ups become unnecessary, but on that first visit the conservative approach protects both your patient and your clinical reputation.
 The corrugator supercilii is the muscle responsible for the vertical frown lines between the eyebrows, and its anatomy directly informs how you should inject because the muscle runs from the periosteum medially all the way up through different tissue layers and fat pads before touching the dermis at its far lateral point. This anatomical course means you should inject deeper medially and become more superficial as you move laterally along the brow, which simultaneously reduces your side effect risk and improves your product efficiency.
The corrugator supercilii is the muscle responsible for the vertical frown lines between the eyebrows, and its anatomy directly informs how you should inject because the muscle runs from the periosteum medially all the way up through different tissue layers and fat pads before touching the dermis at its far lateral point. This anatomical course means you should inject deeper medially and become more superficial as you move laterally along the brow, which simultaneously reduces your side effect risk and improves your product efficiency.
Eyelid ptosis from botox is most commonly caused by corrugator injections, specifically because as you inject more laterally you get closer to the supratrochlear foramen where an artery and nerve run through the septum, and if toxin reaches the levator palpebrae superioris through this route then the eyelid muscle relaxes and a ptosis develops. The anatomical advantage of injecting more superficially at the lateral point is that the fat pad sits between your needle and the foramen, creating a physical barrier that reduces this risk while still delivering an effective treatment.
The question of whether you should always treat the corrugator when treating the frontalis has a nuanced answer that depends on understanding vectors. As a general rule the two should be treated together, because if you relax the frontalis which normally lifts the brow upward but leave an untreated corrugator with a strong downward vector, the patient can end up with a much more aggressive frown than they had before treatment. Patients often describe this as their partner thinking they look angry when they are not, because that subtle interested expression suddenly becomes something much more severe when the upward counterbalance has been removed. With experience and careful vector analysis you can identify patients who genuinely do not need corrugator treatment because their frown vector is relatively flat, but the default position for less experienced injectors should be to treat both areas together.
The procerus runs down the bridge of the nose and pulls the glabella downward, and the most clinically relevant thing about it is the enormous variation between patients, ranging from essentially absent with no visible downward movement to being the dominant muscle in the frown complex with very little corrugator action at all. This means injecting the same number of procerus units on every patient virtually guarantees you are either wasting product or under-treating on any given appointment, and a patient with a dominant procerus might need 12 units there with very little into the corrugator while another patient might need almost nothing.
One clinical application that connects procerus treatment to non-surgical rhinoplasty is the observation that in patients with a strong procerus, the downward pull can create a bend exactly on the part of the nose that presents as a bump, and even after correcting this with dermal filler the movement restores some degree of the bump you were trying to eliminate. Relaxing the procerus with toxin before placing filler gives the product a more stable surface and may help the filler last longer, making it worth considering even in patients who are not presenting with any concern about lines or wrinkles.
 The orbicularis oculi is a circular muscle running close to the surface all the way around the eye, and the multiple vectors involved in a circular muscle make it considerably more complex than treating lateral canthal lines alone might suggest. Relaxing the lateral aspect can unmask a medial pull that was previously neutralised by the opposing lateral vector, and if you chase those medial lines with more toxin the problem can worsen to the point where every small smile produces a visible and unnatural-looking medial contraction, which is one of the recognisable botox signs that makes patients look overtreated.
The orbicularis oculi is a circular muscle running close to the surface all the way around the eye, and the multiple vectors involved in a circular muscle make it considerably more complex than treating lateral canthal lines alone might suggest. Relaxing the lateral aspect can unmask a medial pull that was previously neutralised by the opposing lateral vector, and if you chase those medial lines with more toxin the problem can worsen to the point where every small smile produces a visible and unnatural-looking medial contraction, which is one of the recognisable botox signs that makes patients look overtreated.
The orbicularis oculi exists in a tug of war with the frontalis, pulling the brow downward while the frontalis pulls upward, which is why relaxing the orbicularis can produce a subtle brow lift and has even been used to partially correct a brow ptosis caused by over-treating the frontalis. In the lower portion the muscle acts as an accessory to cheek elevation, and over-treatment here can flatten the duchenne smile, that genuine full-face smile our brains instinctively recognise as authentic, making the patient’s expressions look less natural.
The single most effective technique improvement for crow’s feet injection depth is to inject far more superficially than most clinical training instils, with the needle inserted perhaps a millimetre and a half so it sits just on top of the muscle. This minimises bruising and keeps the muscle itself as a shield between the toxin and the deeper zygomatic muscles, because affecting those muscles produces an asymmetry in the smile that looks like a stroke and is one of the most distressing botox complications a patient can experience.
In older patients the stakes are higher still because the muscles are doing more structural work holding the lower face together, and over-treating the orbicularis to chase lines can cause the cheek to sag and actually make the patient look older, which underscores why sometimes the right clinical decision is to use less toxin and address the remaining concerns through other modalities such as dermal filler.
Join us for one of Dr Tim's FREE upcoming webinars.
Check dates here and save your spot

Dr Tim Pearce MBChB BSc (Hons) MRCGP founded his eLearning concept in 2016 in order to provide readily accessible BOTOX® and dermal filler online courses for fellow Medical Aesthetics practitioners. His objective was to raise standards within the industry – a principle which remains just as relevant today.
Our exclusive video-led courses are designed to build confidence, knowledge and technique at every stage, working from foundation level to advanced treatments and management of complications.
Thousands of delegates have benefited from the courses and we’re highly rated on Trustpilot. For more information or to discuss which course is right for you, please get in touch with our friendly team.





