You may be interested




 Dr Tim Pearce
Dr Tim Pearce

Picture the scene…You are treating a patient with dermal filler, and they start to lose their sight, right there in front on you. What do you do? This is a scenario that strikes terror into every aesthetic clinician, no matter how experienced they are, but being prepared for such a worst-case event, ahead of time, will help you to avoid panic should it happen to you.
In this blog, Dr Tim Pearce will examine the options available in that critical moment. He discusses whether a retrobulbar injection of hyaluronidase is the right course of action, or a peribulbar approach, or if frankly, it is best left well alone.
Dr Tim will be discussing more medical aesthetic training tips as part of his upcoming webinar series, so if you’re looking to increase your CPD-certified learning and want to learn more skills to make you a better practitioner, then step one is to register for the free webinars by Dr Tim.
Blindness caused by dermal filler injection
Causing blindness with dermal fillers is an incredibly rare event, thankfully. Data suggests that it may occur in approximately 1 in 300,000 cases, which is around ten times less likely than being involved in a serious car accident.
Despite the risk of causing this complication being very low, it is still beholden on aesthetic clinicians to prevent or mitigate its occurrence and be prepared in the event of a need for management of an ocular compromise.
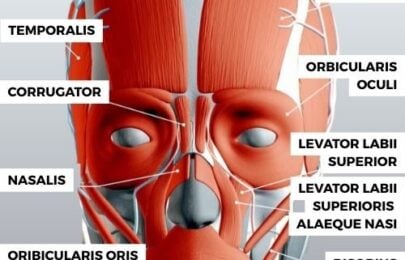
The risk of causing blindness with dermal filler injections is increased when injecting near vessels which are derived from the internal carotid blood supply. The ophthalmic branch of the internal carotid comes out through the orbit and has connections to the supratrochlear, the supraorbital, the lacrimal, and the angular arteries, the latter often having a direct connection to the supratrochlear artery.
This anatomy dictates that dermal filler injections to the forehead, the glabella, the naso-labial folds, and the nose for non-surgical rhinoplasty carry the most risk of causing blindness. Although incredibly rare, cases have been seen generated from treatment elsewhere in the face, including the chin.
Vision loss and damage to the eye from filler injection
 Should the retina of the eye be starved of blood, it will not last very long before damage becomes irreversible. Animal studies suggest a maximum of 90 minutes to resolve ocular compromise before the chances of restoration are lost.
Should the retina of the eye be starved of blood, it will not last very long before damage becomes irreversible. Animal studies suggest a maximum of 90 minutes to resolve ocular compromise before the chances of restoration are lost.
Diagnosis should, in theory, be speedy in such cases because the patient is likely to rapidly report concerns about a loss of their vision. Therefore, if there is a time to save the retina in severe cases, the clock is ticking, and that time is early on.
With the knowledge of how quickly the ocular impairment can become permanent, would you do the risky procedure of administering a retrobulbar injection of hyaluronidase?
What is a retrobulbar injection of hyaluronidase?
The theory behind delivering a retrobulbar injection of hyaluronidase is to place the hyaluronidase as close as possible to the ophthalmic and retinal arteries as the best option for rapid restoration of vision.
The procedure involves an injection technique most commonly employed during the delivery of anaesthesia for ophthalmic surgeries. This is an inherently risky place to put a needle, but the aim is to place the enzyme behind the eye, directly in the vicinity of the blocked or compromised vessels, whilst also avoiding damage to other critical structures nearby, such as the globe of the eye, the nerve, or the blood vessels around the eye.
Steps to administer a retrobulbar injection of hyaluronidase
- Step 1
Compress the eye to shift the globe of the eye upwards, so that it is higher up in the orbit, to create more potential space inferiorly so that you can pass the needle. - Step 2
Common techniques suggest angling your needle for the first 2 millimetres at approximately 120° until you hear a popping through the orbital membrane. - Step 3
At this point you can rotate the needle until it is at 90° to the facial plane before inserting a further 12-15 millimetres. At this depth, the needle tip is deep enough that the eye is curving rapidly away from the needle point. - Step 4
The angle can be changed again, back to 120°, whereupon you are resting the base of the needle on the orbit. Slide the needle in a further 15 millimetres. Your needle will now be inserted by a total of approximately 30 millimetres. This will position it behind the eye and in the target location for hyaluronidase delivery. Any deeper and you risk damaging the optic nerve and compromising other blood vessels. - Step 5
Now you are in position, you can inject up to 3mls of hyaluronidase solution. The theory behind this restriction on the volume delivered is that the globe is in an enclosed space, thus if you inject more than 10-15% of the volume of the globe, you can compress the structures causing additional damage.
Should you perform a retrobulbar injection of hyaluronidase?
The question we now need to ask is, should the average aesthetic clinician perform a retrobulbar injection in the event of an emergency involving vision loss?
There are many factors to consider when attempting to answer this question. We must think about the risk of the procedure versus the benefits of the procedure, and compare those to the risk of not treating, or to applying other rescue treatments, such as a peribulbar injection technique.
The risk associated with retrobulbar injections include injury to the globe such as piercing (1 in 12,000), retrobulbar haemorrhage (1.7%), optic nerve damage, extra ocular muscle injury, and central spread of local anaesthetic if you mix the hyaluronidase with lidocaine (which is not recommended).
The reality of this procedure is that even in the hands of trained ophthalmic professionals, it can be very difficult to place product accurately. This is reinforced by some clinical studies (predominantly related to anaesthesia placement for ophthalmic procedures) that showed that only half of the injections were in the intraconal space. Such evidence makes it very difficult to recommend this as an emergency course of action for all aesthetic clinicians.
Diagnosis can be a problem in these cases too, with many grey areas including false reporting from the patient linked to anxiety and panic attacks, partial disturbances in vision loss which can recover with little to no medical intervention, or transient vision loss which may be related to spasms in certain vessels, rather than occlusion. The patient may also have undisclosed pre-existing or undiagnosed visual problems which may manifest and cause complexity.
At the end of the day, most aesthetic clinicians are relatively inexperienced at treating patients with sudden onset blindness. This makes for a high stress situation which can impede their ability to make clear decisions; they may be overeager to attempt a risky emergency protocol, whereas a more experienced clinician may hold back and evaluate the situation, minute-by-minute, to determine the most appropriate action plan. Rushing to treat in a panic can have serious medico-legal consequences.
Is peribulbar injection of hyaluronidase an option for filler blindness?
An alternative option would be to consider a peribulbar injection of hyaluronidase. This technique is not as deep as a retrobulbar approach – you only advance the needle to around the equator of the globe and without any rotation needed to reach the posterior space. This means that there is less chance of injury to the optic nerve or other vessels which could result in a retrobulbar haematoma, a significant complication in itself. This technique has the advantage that it places you closer to the vessels, superiorly, that are likely to have been occluded by the dermal filler injection, i.e., the supratrochlear, the supraorbital, and the lacrimal arteries.
It is important to conclude this blog by noting that Dr Tim is not recommending that every patient who has visual disturbance after a dermal filler injection needs a retrobulbar injection of hyaluronidase. There is a lack of evidence to back this up as a helpful option and there is concern that it could make the situation worse. The important take-home message is that these situations are not black and white; differential diagnosis plays a part in the problem, which could outweigh any benefits of emergency intervention.
Dr Tim’s advice is that aesthetic clinicians should familiarise themselves with blindness as a potential complication of filler treatment, learn the approaches to treat it and the anatomy by perhaps investing in a cadaveric masterclass. Only then can you evaluate for yourself what would be the best approach in each situation – should the worst happen one day.
Of course, mitigating the risk of causing blindness with your dermal filler injections is by far and away the best message to take from this. Why not download Dr Tim’s Facial Vessel Map with the 13 extra risky injection areas.
Aesthetics Mastery Show
RED NOSE TIP COMPLICATION. Pressure necrosis after non-surgical rhinoplasty
This blog follows our recent Aesthetics Mastery Show, in which Dr Tim Pearce discusses the 8 different mechanisms by which vascular injury after dermal filler can cause necrosis.
Are you still anxious about delivering cosmetic injectables safely?
If you want to learn more about mastering medical aesthetic treatments and complications or conquering the anxiety of where to place your needle, then register for the next Dr Tim webinar.
Subscribe to our YouTube channel for really useful regular tips and advice. ![]()
Dr Tim Pearce eLearning
Dr Tim Pearce MBChB BSc (Hons) MRCGP founded his eLearning concept in 2016 in order to provide readily accessible BOTOX® and dermal filler online courses for fellow Medical Aesthetics practitioners. His objective was to raise standards within the industry – a principle which remains just as relevant today.
Our exclusive video-led courses are designed to build confidence, knowledge and technique at every stage, working from foundation level to advanced treatments and management of complications.
Thousands of delegates have benefited from the courses and we’re highly rated on Trustpilot. For more information or to discuss which course is right for you, please get in touch with our friendly team.