




FREE Complications Webinar
Want to overcome your fear of complications and confidently master anatomy?
Join us for one of Dr Tim's FREE upcoming webinars.
Check dates here and save your spot
 Dr Tim Pearce
Dr Tim Pearce
The fat pads of the face divide into superficial and deep compartments, with the division generally occurring at the superficial musculoaponeurotic system layer that separates these two compartments though the mid-face presents more complexity than this simple model might suggest. Understanding where these deep fat pads sit relative to the SMAS and how they function both structurally and aesthetically becomes essential for practitioners who want to design treatment plans that restore facial architecture in ways that patients can understand and trust when making decisions about dermal filler procedures.
Fat pads perform three primary roles in the face beyond the purely biochemical function of producing energy when the body needs it, which represents the least interesting aspect from an aesthetic perspective. The functional component means that fat pads provide a degree of support for the muscles so they don’t sag as easily, while they provide a point of leverage so that a smaller contraction might pull more tissue more easily, and they also dampen muscle movement so that a contraction isn’t overly overt which creates a harmonizing effect across facial movements.
This harmonizing function leads into the secondary category where these fat pads create an aesthetic difference, and the way to think about aesthetics involves recognizing that beauty fundamentally projects health to observers. What we call beauty effectively communicates health, and those fat pads convey a sense of health when they’re in the right place at the right volume, creating what we perceive as an attractive individual. The function of the face becomes almost a social skill in this context, operating as a social survival mechanism where looking healthy maximizes opportunities for connection and success.
When you search for deep fat pads online you’re going to encounter a recurring image showing the primary deep fat pads, though more detailed images exist that reveal additional compartments. Some papers discuss four or five compartments just in the forehead region including the subprocerus or galeal fat pad, along with subfrontal deep fat pad compartments underneath the frontalis muscle, adding up to five deep fat pads underneath the frontalis muscle that become important for forehead shaping and volume restoration. Around the eyes we mainly discuss the suborbicularis oculi fat pad which divides into two different fat pads called the lateral and medial SOUF, and this distinction becomes very important for tear trough treatments since this represents what we restore when treating the tear trough area.
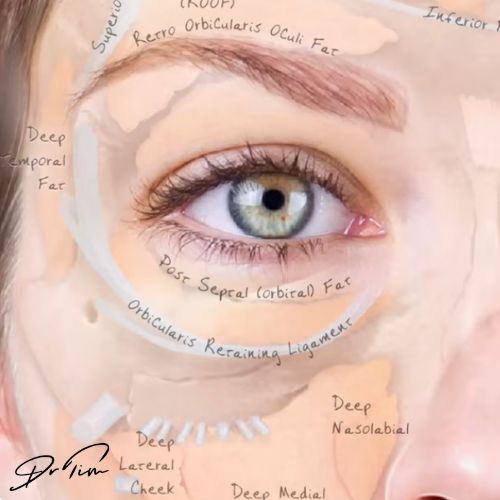
The mid-face presents more complexity than most internet images suggest, with most diagrams showing two main fat pads including the buccal fat pad which extends all the way underneath the zygoma into the temple, and the deep medial cheek fat pad. More detailed descriptions include the deep lateral cheek fat pad and the deep nasolabial fat compartment which sits in the pre-maxillary space on top of the levator labii superioris alaeque nasi muscle. This anatomical relationship matters because the mid-face differs from the lateral part of the face in that deep fat pads can lie on top of muscles due to this roof tile effect, creating an unusual arrangement where even though a fat pad sits deep there may sometimes be muscles underneath it.
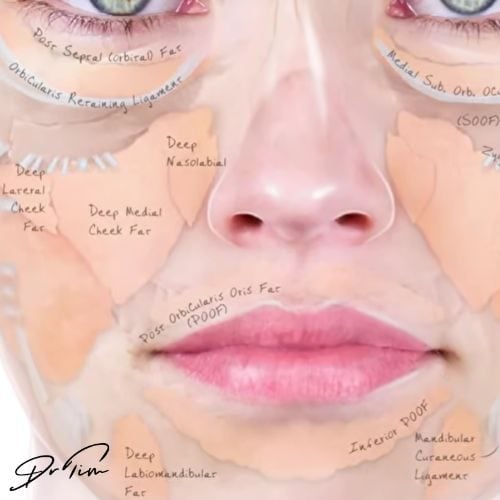
Most textbooks don’t discuss the deep fat pads much in the lower face, but digging into the research reveals evidence that a deep fat pad compartment exists in the lower face as well. The retro orbicularis oris fat pad appears particularly relevant when examining very old faces where you can observe much less volume in the whole structure around the mouth, and these deep fat pads become useful with more holistic restorations when taking years off someone’s appearance.
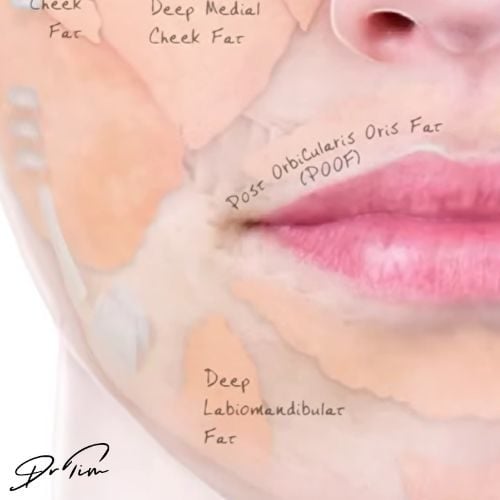
The deep chin fat sits medially right in the middle of the chin underneath the mentalis muscle, and the deep labiomental fat pad sits lateral to that structure, with these components making up the lower face deep architecture that remains important for stabilizing the position of the chin. Treatments performed relatively deep with a cannula can help restore the chin which functions like the cherry on the bottom of the face, giving that heart-shaped facial appearance when you have a chin that ends at the low point of the face.
The decision about whether to inject superficial or deep fat pads depends on the specific clinical situation, though in many places practitioners often start with deep injections since you’re usually restoring the underlying structure when looking at a face. In practice you’re injecting all of the fat pad layers in most comprehensive treatments, layering with some injections placed deep and some placed superficially, with a common approach involving doing a first pass deep and then picking up smaller details with more superficial cannula work in certain parts of the face.
Understanding deep fat pads provides a helpful framework for patients to understand that there’s an anatomical basis for what they see in the mirror, and when they can relate a deficit which makes them feel a certain way to anatomical change that you can directly repair by replacing the lost volume, that becomes a very neat story in the mind of someone who wants to look natural. This makes discussing fat pads incredibly useful in the consultation process, and there’s also a sound basis for your treatment recommendations when you can explain the anatomical reasoning behind your proposed approach.
This scientific foundation doesn’t matter to everyone since some people don’t really care about the science and just trust you to do what you think is best, though most injectors don’t have that luxury. You need to present a case about why you’re going to treat your patient in a certain way to win their confidence, and presenting why you recommend a specific treatment based on fundamental anatomical ideas creates a persuasive rationale that patients can understand.
Once you understand the anatomy of the fat pads it becomes quite clear where you need to inject and how much you need to inject. Taking temples as an example, the deep temple fat pad and the buccal fat pad form quite a large structure measuring about 15 milliliters in normal youth, though this volume shrinks significantly as you get older which creates the temporal hollowing that ages the face.
When recommending a treatment and discussing volumes with patients, having these baseline numbers becomes useful since knowing that your normal buccal fat pad measures 15 milliliters means that placing two milliliters doesn’t represent a very large treatment even though it might seem substantial without that anatomical context. The most common spectrum of temple treatment runs from about half a milliliter on each side up to two milliliters on each side, though you can probably go as high as four milliliters on each side in some individuals if not even higher.
Fat changes represent one of the primary transformations that occur with aging, but where the anatomy really gets interesting involves how we relate these fat pads to the ligaments that attach the skin to deeper structures. The ligaments run through these fat pads and create potential spaces which change as you get older, so lost volume or excess volume combined with the ligaments means you can start to see little dips in the skin where the skin is held down by these retaining structures.
This relationship between superficial fat, deep fat, and the ligaments possibly accounts for 70 to 80 percent of what you’re actually seeing in terms of facial aging. Most of the shadows that appear in your face are basically caused by ligaments serving as break points where fat pads shift position, with the orbicularis oculi retaining ligament creating your tear trough, the zygomatic ligament crossing your cheek, the nasolabial fold having an attachment-like ligament, and the melolabial fold caused by the mandibular retaining ligament.
These structures function as break points where the fat pad shifts and causes that little shadow that marks the transition between different tissue planes, and explaining this to patients during consultations demonstrates your anatomical knowledge while helping them understand why you’re recommending specific injection sites and depths. When you present the case as if you’re trying to convince a colleague why they should have the treatment, your trust levels go through the roof because they’re actually learning something and while they’re learning you’re demonstrating your authority and knowledge in a way that builds genuine confidence in your recommendations.
Join us for one of Dr Tim's FREE upcoming webinars.
Check dates here and save your spot

Dr Tim Pearce MBChB BSc (Hons) MRCGP founded his eLearning concept in 2016 in order to provide readily accessible BOTOX® and dermal filler online courses for fellow Medical Aesthetics practitioners. His objective was to raise standards within the industry – a principle which remains just as relevant today.
Our exclusive video-led courses are designed to build confidence, knowledge and technique at every stage, working from foundation level to advanced treatments and management of complications.
Thousands of delegates have benefited from the courses and we’re highly rated on Trustpilot. For more information or to discuss which course is right for you, please get in touch with our friendly team.





