




Note:
This article was written by a guest contributor from our community. The views and clinical opinions expressed here belong to the author and do not necessarily reflect the opinions or endorsements of Dr Tim Ltd.
 Dr Tim Pearce
Dr Tim Pearce
 Dr. Nieves Romero – Dermatologist
Dr. Nieves Romero – DermatologistDr. Nieves is a medical doctor with a strong interest in aesthetic and regenerative medicine, focused on evidence-based and holistic approaches to skin health. Her work emphasizes understanding the skin as a reflection of internal balance, combining medical treatments with nutrition, lifestyle strategies, and preventive care to achieve natural and long-lasting results. She is passionate about continuous learning, scientific communication, and sharing knowledge that bridges clinical practice with modern aesthetic medicine.
https://instagram.com/dra_nievesromero
Melasma is an acquired cutaneous disorder characterized by hyperpigmentation of sun-exposed areas of the skin, significantly affecting the quality of life of those who suffer from it. It occurs more frequently in individuals with Fitzpatrick skin phototypes III–IV, although lighter phototypes may also be affected. The convex areas of the face are predominantly involved; however, the neck, chest, and arms can also be affected to a lesser extent.
Diagnosis is primarily clinical, although complementary tools such as Wood’s lamp examination and dermoscopy can help assess the depth of pigmentation and guide appropriate treatment strategies. Skin biopsy is rarely indicated, as histopathological findings are often nonspecific.
Multiple factors—including hormonal influences, genetic predisposition, and phototype—contribute to its complex etiopathogenesis. The often-poor response to treatment and high recurrence rate, make melasma a true therapeutic challenge, frequently leading to frustration for both patients and clinicians.
The gold-standard therapy remains the combination of hydroquinone, fluocinolone acetonide, and tretinoin for at least six months, followed by consistent photoprotection. However, more recently, multimodal approaches integrating intradermal therapies (such as mesotherapy or microneedling with topical actives), energy-based devices (including laser treatments), and off-label oral agents like tranexamic acid have demonstrated promising results.
A 36-year-old female patient attended the clinic on her own initiative, reporting the following history: Gyneco-obstetric history: irregular menstrual cycles, use of oral contraceptives, two pregnancies, two deliveries. No other relevant findings on medical interview.
She consulted for facial lesions of seven years’ evolution, which she associated with her first pregnancy and sun exposure. The condition presented with local symptoms such as facial warmth and occasional pruritus. She also reported having undergone inconsistent treatments without effective results.
Physical examination: hyperpigmented macular lesions predominantly located on the convex and photoexposed facial areas — forehead, cheeks, perioral area, and nasal region — over mildly erythematous skin, warm to the touch.

Dermatoscopy: in the hyperpigmented areas, a brown pseudo-network with irregular distribution was observed, with preserved follicular openings and pigment surrounding polygonal telangiectasias.
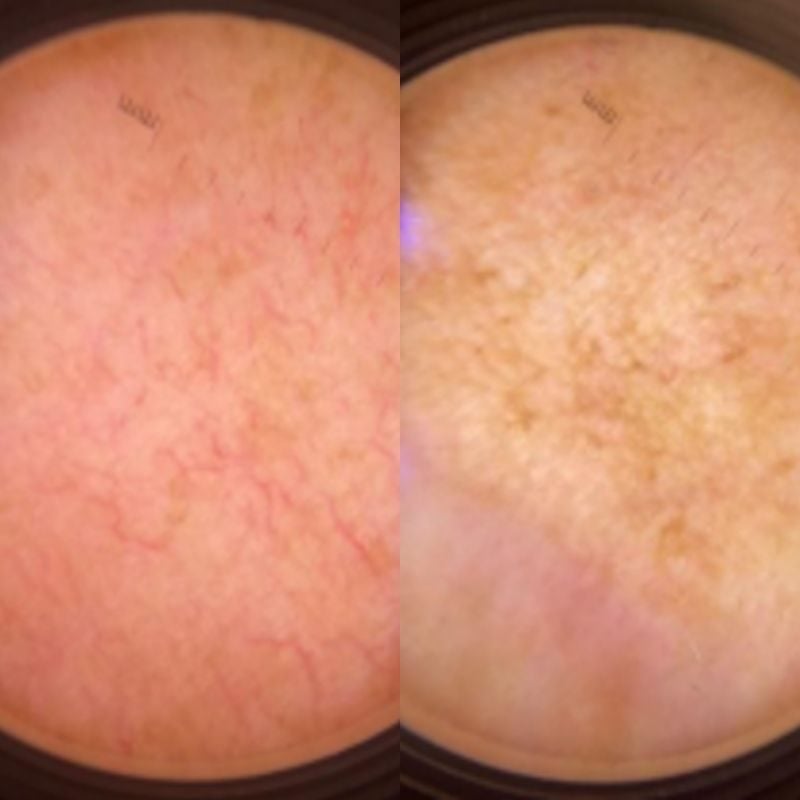
Wood’s lamp examination: enhancement of melanin pigment on the cheeks.

1. Epidermal melasma, centrofacial type.
2. Erythematotelangiectatic rosacea.
Given the patient’s symptomatology (local heat, burning sensation, and pruritus), it was decided to initially address rosacea with the following treatment plan:
1. Topical ivermectin 1%, nightly.
2. Topical decongestants or thermal water containing Hamamelis, Aloe vera, and Sepicalm.
3. Sunscreen SPF 50, applied every two to three hours.
Significant improvement in rosacea, with reduction in erythema, local warmth, and subjective symptoms.
Melasma treatment was then initiated as follows:
1. Continue sunscreen use and standard skincare measures.
2. Home topical treatment with tranexamic acid cream combined with niacinamide, vitamin C, sunscreen, and Uva ursi, applied nightly.
3. In-office management: facial mesotherapy every 15 days with a combination of tranexamic, retinoic, and phytic acids, alternating with chemical peels using 30% mandelic acid.
4. Oral tranexamic acid 250 mg twice daily.
Slight improvement in hyperpigmentation was noted. The treatment was continued for two more months with periodic evaluations.
The infiltration formula was alternated with kojic acid, and chemical peels were discontinued, maintaining in-office facial infiltrations along with previous recommendations (home topical treatment and sunscreen).
Oral tranexamic acid was discontinued in the third month due to patient intolerance.
At six months after treatment initiation, marked improvement was observed with no recurrence and patient satisfaction. Comparative photographs were taken.

The patient remains under periodic follow-up, with regular use of sunscreen, topical decongestants for rosacea control, and general skincare measures.

This article was written by a guest contributor from our community. The views and clinical opinions expressed here belong to the author and do not necessarily reflect the opinions or endorsements of Dr Tim Ltd.
Dr Tim Pearce MBChB BSc (Hons) MRCGP founded his eLearning concept in 2016 in order to provide readily accessible BOTOX® and dermal filler online courses for fellow Medical Aesthetics practitioners. His objective was to raise standards within the industry – a principle which remains just as relevant today.
Our exclusive video-led courses are designed to build confidence, knowledge and technique at every stage, working from foundation level to advanced treatments and management of complications.
Thousands of delegates have benefited from the courses and we’re highly rated on Trustpilot. For more information or to discuss which course is right for you, please get in touch with our friendly team.





