You may be interested





 Dr Tim Pearce
Dr Tim Pearce
A recent trend you might have seen on Instagram has aesthetic practitioners taping up their patients’ lips after filler injections, claiming it prevents migration and creates better definition. The technique looks compelling on social media. But does the science support these claims? Let’s break down the tissue integration evidence, safety concerns, and what practitioners need to know before offering this technique.
What actually is lip taping?
Clinicians take a steri-strip or some other form of tape and structure it around a lip in a specific way. Usually, they’re everting the lip and laying strips of tape around areas where they want to create a straight line. The visual implication suggests they’re creating external rotation and definition along the lip, then holding it in place for a certain period of time.
One of the more interesting claims about this technique is that it might prevent migration.
The migration prevention claim: Does it hold up?
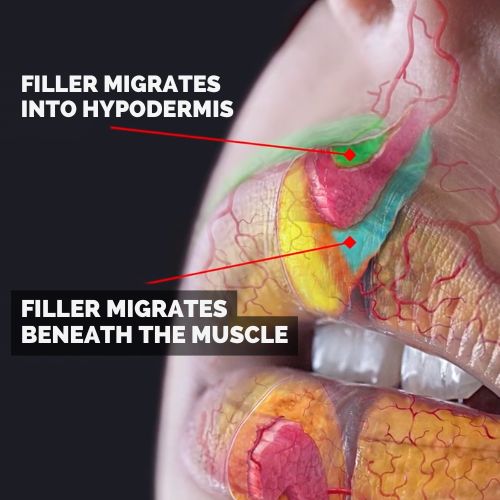
Think about what’s actually going on in the lip when you have migration. Typically, product has been injected in an area where it’s very easy to diffuse. For example, if you inject directly on the vermilion border where the muscle inserts into the border, it will essentially spill over onto either side of that insertion point. You’re not actually putting the filler in one compartment, you’re putting it on the border between two compartments.
If you were to put tape on top of that situation and leave it there for 24 hours, it’s likely that it would have very little impact on the chances of that actually spreading over time. It may delay it a little bit.
This gets to the heart of what’s implied by this technique: the idea of tissue integration.
The tissue integration question nobody can answer
If you put filler in a place and hold it in that place until it sets, will it stay there for longer?
There’s a lot of detail in that claim that needs unpacking. We actually don’t know how long it takes most fillers to set. We also don’t know if it does set exactly, or how strong that set actually is. We know it’s not concrete.
The idea that you could hold filler in a particular position and then it would be more likely to stay in that particular position could be true if it’s held well. But how long it will stay there is completely unknown.
The wide variation in filler integration
When you look up tissue integration, you’ll find wide variation between fillers. Some integrate to some degree. Some integrate much, much less.
We also know this from extrusion of fillers. Imagine taking a dermal filler lump and putting a needle in and squeezing it. We know we can squeeze filler out quite easily – If you can squeeze filler out through a hole made by a 23 gauge needle, then you’re almost certainly dealing with a filler that is not integrated into the tissue.
This has massive implications for lip taping. If you simply have a bubble of filler that you’re holding in place so that when you remove the tape it seems to have done something, you’ve actually achieved nothing in the long arc of time. It’s going to do what it would have done afterwards. The most important element would have been: did you inject it into the right compartment?
The extreme argument: No integration equals pointless taping
If we say there’s no tissue integration, or almost none, let’s say it’s 90% not integrated, then there’s absolutely no point taping the lips. It might look good for a second or two, maybe even 30 minutes after you remove it. But it’s going to settle to its more neutral position.
What would have mattered most is exactly where you injected it, not what you did with the tape.
The moderate argument: Some integration, temporary results
The other side could be that there is some tissue integration. Let’s presume that some fillers integrate 90%. We still don’t know exactly how strong that structure is.
If it was to set like concrete, you could just shape it exactly how you wanted, release it, and it would stay that way. But that’s not necessarily how filler works. There’s probably a little bit of that, but it’s not going to be strong enough that holding it for 24 hours means it’s just going to stay that way.
Based on how long dermal fillers tend to hold their shape, you might get an initial result that fades very rapidly, probably within a day or two.
The visual story is very compelling, but there are a lot of unknowns about whether this actually makes any difference to the patient.
Where this idea actually came from
The idea in its essence is not new. People have been using dental floss to illustrate the keyhole lip technique. They run dental floss between the front two teeth, pull it down, and inject on either side.

This creates a visual story that if you inject filler, it will stay on one side if the dental floss is there. By implication, if the dental floss wasn’t there, it would instantly flow to the other side and ruin your shape.
That same idea is at play with lip taping. It superficially makes sense if you have a mental model that filler is just flowing haphazardly into tissues with no boundaries. There’s no anatomy. It’s literally just like plasticine that you’re shaping.
An understanding of anatomy would show that it simply isn’t how the filler flows. It tends to be restrained within compartments. It doesn’t need a piece of dental floss to hold it in one compartment or the other. You can just shape it the way you want it and inject where you want it to be.
If it does flow, you could squeeze it and then it would stay in the same place. But you don’t need to hold things in place.
At the bottom of this is the same idea. It’s an understanding of filler that it’s like plasticine you can shape any way you want, and it should stay that way, but it’s not entirely true. Think more in terms of compartments, depth, and position of injection.
There is a grain of truth in the shaping concept, but it’s likely over-emphasised with these two different methods of communicating to patients on Instagram.
Safety concerns with lip taping
With the typical techniques, if there’s not a lot of pressure on the lips, there’s no particular safety concern.
Dry mucosa from extreme eversion
One of the most subtle things that could happen: if you tape a lip outwards, and a lot of these techniques tape so much that you can see them everting the lips significantly, you will rotate the wet-dry border outwards. You’re effectively exposing the internal mucosa of the mouth to the elements.
That’s going to be very irritating for patients. The oral mucosa is going to be drying out. It won’t be fun living like that constantly, either applying vaseline or licking your lips to get through a day if it was to last that way.
It’s more the extreme of external rotation that stands out as a potential risk.
Blood supply restriction
The other risk is that if it’s taped tightly enough, you could restrict blood supply. But it’s more likely the opposite – putting so little pressure on that it’s not really changing the position that much.
But if you did put enough pressure, and particularly if it was taped backwards and there was a bend in the skin, pressure for a long period of time on tissue is not good for it.
The hidden complication risk
There’s another risk his producer recently pointed out: if you’ve covered up the area you’ve just injected, there’s a chance you may misdiagnose complications. Certainly patients may be less likely to report or to see discoloration.
Perhaps even if there’s pain, they may put it down to the tape. They might not realize they have a vascular occlusion.
This is worth considering if you’re going to tape up the area. You’re going to deprive yourself of certain amounts of information. Very similar to the scalp necrosis cases that we see, it becomes harder to diagnose when you simply can’t see capillary refill.
A lot of this is going to hide the patient’s self-diagnosis and the clinician’s ability to diagnose without taking all the tape off. In certain circumstances, it could lead to a worse outcome for patients and a worse complication management profile.
The biggest risk: Creating a false story
The biggest risk overall is that it creates a false story. It’s a very compelling story, but it’s not necessarily true. We never get to see what happens to these patients three months down the line and how they feel about their product at that point. No one puts those failures onto Instagram.
You just see the initial taping up. Everyone gets it quickly because it’s very visual, but you don’t know what happens next.
The truth is your only friend in the long run
It is much better to be aligned with something that’s true, even if it’s less powerful, than it is to make a big claim and then find out that it’s really quite 5 out of 10 or even less, and your patients are disappointed.
If you break trust with your patients, you lose everything.
What you can learn from this trend
Visual explanations are super powerful and what we can take from this is that people really value these visual representations of things they are pursuing.
Maybe there are other ways you can convey things that are more true that you do for your patients using visual explanations.
The fine line between marketing and making up stories
There’s always a fine line between bringing something to market and making up a story that isn’t actually true. People create anticipation for something. If it meets that anticipation, it’s fantastic.
But quite often, they’ve already paid for it and moved on by the time they’ve realised it’s not really that great.
When you do that with your patients, you are withdrawing from the bank of trust. Be very clear that with your patients – if you’re not sure and you’re doing lip taping, you should tell them you’re not sure.
If you are super enthusiastic about it and say it’s going to be amazing, and they find out three months later that it’s not amazing, you’ve lost the most important asset in your clinic: trust with your patients.
The practitioner’s decision framework
When patients ask about lip taping or when you see this trend on social media, here’s what to consider:
- The scientific evidence
We don’t actually know how long fillers take to “set” or how strong that integration is. The claim that holding filler in place prevents migration has no solid evidence behind it. - The anatomical reality
Filler doesn’t flow haphazardly like plasticine. It tends to be restrained within anatomical compartments. Proper injection technique into the right compartment matters far more than any external tape. - The temporary illusion
You might achieve a result that looks good immediately after removing the tape, but it will likely fade within 24-48 hours as the filler settles to its natural position. - The safety considerations
Extreme eversion can dry out oral mucosa. Tight taping could restrict blood supply. Most concerningly, taping can hide early signs of vascular occlusion. - The trust factor
If you offer this technique with enthusiasm and patients are disappointed three months later, you’ve damaged the most valuable asset in your practice.
The bottom line for aesthetic practitioners
Lip taping looks visually compelling on social media. It tells a clear story that patients can understand. But the story it tells about preventing migration and creating permanent definition isn’t supported by what we know about how fillers actually work in tissue.
You might achieve a temporary result. You might create a great before-and-after photo for social media. But you’re not changing the fundamental behavior of filler in tissue, and you’re potentially hiding complications while they’re still easily manageable.
Think twice about offering this technique, because the claimed benefits don’t quite align with filler behavior, tissue integration, and anatomical compartments.
If you do choose to offer it, be honest with your patients about the unknowns. Tell them you’re experimenting. Don’t promise migration prevention or permanent results you can’t deliver.
Your reputation is built on truth, not on viral techniques that look good for Instagram but disappoint patients three months later.
Watch the full Aesthetics Mastery Show
Should you Offer Lip Taping? What You Need To Know About the Tiktok Trend
In this episode Dr Tim addresses the Tiktok Lip Taping trend. He shares his thoughts on the treatment, so you can make a decision on whether you should offer it to your patients
You can also subscribe to our YouTube channel for really useful regular tips and advice. ![]()

Dr Tim Pearce eLearning
Dr Tim Pearce MBChB BSc (Hons) MRCGP founded his eLearning concept in 2016 in order to provide readily accessible BOTOX® and dermal filler online courses for fellow Medical Aesthetics practitioners. His objective was to raise standards within the industry – a principle which remains just as relevant today.
Our exclusive video-led courses are designed to build confidence, knowledge and technique at every stage, working from foundation level to advanced treatments and management of complications.
Thousands of delegates have benefited from the courses and we’re highly rated on Trustpilot. For more information or to discuss which course is right for you, please get in touch with our friendly team.
Dermal Filler & Lips eLearning Courses
If you want to increase your knowledge about safe and effective lip filler injectable treatments, Dr Tim Pearce offers a series of fabulous courses, from foundation and upwards:
- 8D Lip Design
- Elective Lip Reversal
- Dermal Fillers Foundation Course
- Dermal Filler Complications Mastery
In addition, browse our FREE downloadable resources.





