



FREE Complications Webinar
Want to overcome your fear of complications and confidently master anatomy?
Join us for one of Dr Tim's FREE upcoming webinars. .
Check dates here and save your spot
 Dr Tim Pearce
Dr Tim Pearce
 The debate about vertical versus horizontal lip injection techniques creates unnecessary anxiety for practitioners when the real conversation should center on something far more fundamental to patient safety and treatment outcomes. Some time ago, during a discussion with another well-known injector, a disagreement emerged about where the labial artery sits in relationship to injection technique, and this conversation highlighted how one particular paper concluded that vertical injections might carry more risk than horizontal approaches, which prompted a deeper investigation into why anatomical descriptions can seem so contradictory when examining the same structures.
The debate about vertical versus horizontal lip injection techniques creates unnecessary anxiety for practitioners when the real conversation should center on something far more fundamental to patient safety and treatment outcomes. Some time ago, during a discussion with another well-known injector, a disagreement emerged about where the labial artery sits in relationship to injection technique, and this conversation highlighted how one particular paper concluded that vertical injections might carry more risk than horizontal approaches, which prompted a deeper investigation into why anatomical descriptions can seem so contradictory when examining the same structures.
The claim surfaced during this discussion that the labial artery runs in the wet-dry border, which created significant uncertainty because this positioning seemed dramatically different from the mental picture that had been guiding clinical decisions for years. This experience happens frequently to new injectors who finally feel they understand something about lip anatomy, only to have someone notable or well-respected present completely different information that triggers a mini earthquake in their clinical understanding, leaving them wondering whether everything they thought was true might actually be wrong.
Diving into the details of various papers about anatomy and artery positioning revealed something genuinely helpful for practitioners struggling with these seemingly conflicting descriptions, which is that a lot of anatomical terminology becomes misleading when trying to describe very complex three-dimensional structures using two-dimensional words. The best example of this linguistic confusion centers on wet-dry border versus vermilion border positioning, where some papers categorically state the labial artery sits at the level of the wet-dry border while others declare with equal certainty that it resides in the vermilion border, and this apparent clash makes it extremely difficult to be certain about artery location based purely on these different written descriptions.
Reference points, scale, and precision form the foundation of this misunderstanding, and the scale of needles provides the perfect illustration of where these descriptions fall apart because the thickness of a needle measures just 0.4 millimeters. When describing something as being at the wet-dry border or in the vermilion border without additional context, the initial reading suggests the artery sits exactly where you’re placing your needle, which actually isn’t the case at all since you can have a distance of four to five millimeters between structures that looks to the untrained eye like you’re injecting precisely where the artery is located.
This represents the fundamental problem of scale combined with a lack of precision in the words used to describe exactly where something sits in three-dimensional space, meaning that vermilion border and wet-dry border function as very vague terms without the additional dimension of depth. Practitioners working in clinics put tremendous effort into being as skilled as possible at reducing side effects and risks while achieving the results their patients want, and when different descriptions of the same anatomical structure create uncertainty, a more three-dimensional understanding of the lip provides much more confidence about being in the right place during treatment.
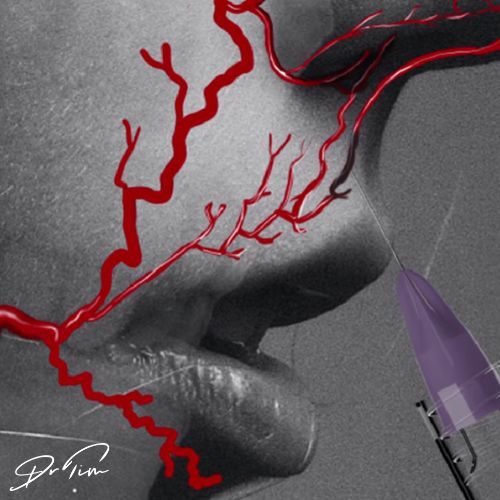
Looking at lip anatomy from a three-dimensional perspective reveals how these seemingly contradictory descriptions can all be correct depending on your viewing angle. If you examine the lip straight on from an anterior view, the artery appears very neatly positioned at the level of the vermilion border, but as soon as you start rotating the view and looking from an inferior angle, the artery relatively appears to move down and deeper because those arteries sit about five millimeters deep within the tissue layers.
Then if you view the structure from the most inferior aspect looking up into the lip, the artery now appears at the level of the wet-dry border, which means both of these different ways of understanding lip positioning are correct simultaneously but what you really need is a combination of both views to develop a much clearer idea of the actual position of the artery relative to your injections. These injections usually run in the anterior third of the lip and therefore occupy a relatively safe place with respect to those arteries no matter which angle you’re injecting at, meaning that whether you use vertical or horizontal approaches, so long as you remain anterior enough in your placement, you should be missing the vessel consistently.
The question of which angle of entry carries less risk matters far less than considering the other factors that determine safety, because both vertical and horizontal approaches can be performed safely so long as depth remains correct. This represents a more important point in many ways than debating which angle you enter at, and the depth of the artery averages about five millimeters in a young lip, though this measurement might change slightly depending on the fullness of the lip and the age of the patient.
Thinking most importantly about depth of needle placement becomes the primary safety consideration, and then there probably exists a small difference in risk between vertical versus horizontal techniques because the artery runs horizontally, meaning you spend more time parallel with it during horizontal injections. Horizontal injections happen all the time in clinical practice and remain safe as long as you maintain correct positioning in all the other ways already discussed, and in terms of actual preference, the shape being created where you tend to be enhancing or at least working close to the vermilion border often makes horizontal injections the more practical choice, though quite superficial placement remains essential.
Occasional vertical injections also have their place in treatment planning, but horizontal approaches probably get used more frequently in actual practice for creating the desired aesthetic outcomes while maintaining appropriate tissue depth. Because of the shape being created where enhancement tends to focus on or near the vermilion border, horizontal injections naturally suit this treatment goal, though remaining quite superficial in the tissue layers prevents any intersection with deeper vascular structures.
Age affects the position of the artery relative to injection approach in ways that demand attention during treatment planning. Picturing a very old person reveals that the lip has elongated over time and some of the pink tissue has rotated back within the lip structure, which means when performing a vertical injection you’re necessarily working at a different angle than when that same person was sixteen years old because they had the pink part of their lip rotated upwards at a younger age.
The angle of entry would be roughly forty-five degrees in a younger patient with good lip projection, but as they age you end up pointing your needle basically behind the muscle where the artery resides. In theory this means smaller lips and older lips require a steeper angle of entry during vertical injection technique, and this positioning ends up with the tip of your needle being closer to the posterior section of the lip where the artery tends to reside, creating additional considerations for safe treatment in this patient population.
The debate between horizontal and vertical injections exists somewhat as a two-dimensional debate when the solution requires three dimensions of understanding. Having access to anatomical descriptions that show the actual position in 3D allows you to understand the crucial relationships that determine safety and effectiveness during injection, because viewing the anatomy from multiple angles simultaneously provides the complete picture you need for confident treatment decisions.
This three-dimensional understanding forms the crucial foundation you need to be safe and effective when injecting lips and to have confidence in your technique based on actual anatomical relationships. Going back to review these anatomical descriptions in 3D helps solidify the mental model that guides every treatment decision, because once you see the spatial relationships between surface landmarks and deeper structures, the anxiety about conflicting terminology disappears and gets replaced with genuine understanding of where everything sits in relation to your needle placement throughout the entire injection process.
Join us for one of Dr Tim's FREE upcoming webinars. .
Check dates here and save your spot

Dr Tim Pearce MBChB BSc (Hons) MRCGP founded his eLearning concept in 2016 in order to provide readily accessible BOTOX® and dermal filler online courses for fellow Medical Aesthetics practitioners. His objective was to raise standards within the industry – a principle which remains just as relevant today.
Our exclusive video-led courses are designed to build confidence, knowledge and technique at every stage, working from foundation level to advanced treatments and management of complications.
Thousands of delegates have benefited from the courses and we’re highly rated on Trustpilot. For more information or to discuss which course is right for you, please get in touch with our friendly team.
If you want to increase your knowledge about safe and effective lip filler injectable treatments, Dr Tim Pearce offers a series of fabulous courses, from foundation and upwards:
In addition, browse our FREE downloadable resources.






