You may be interested




 Dr Tim Pearce
Dr Tim Pearce
Lip filler complications account for over 50% of all aesthetic injection posts in practitioner support groups according to the 2018 ACE group audit of their entire Facebook community, pointing to a reality that makes lips the most frequent area to encounter adverse events despite being among the most requested treatments in aesthetic medicine. The most serious complication remains vascular occlusion while bruising represents the most common side effect, creating a situation where understanding the three-dimensional position of the labial arteries becomes fundamentally essential to protecting your patients from outcomes that can range from tissue necrosis to permanent disfigurement.
Recent research published in the Journal of the American Medical Association studied vascular injury risk in a cohort of dermatologist injectors and discovered a rate of one occlusion occurring every 6,000 milliliters of filler product delivered specifically in lip treatments. The more revealing finding shows that risk decreases as the injector gains experience, with practitioners demonstrating 70% less chance of causing a vascular occlusion after five years of practice, which represents genuinely encouraging news since it proves that the nuances of injection technique affect risk beyond just the anatomical area we inject or the specific methodology we employ.
Understanding what experienced injectors do differently
The question worth exploring centers on what experienced practitioners are doing that inexperienced ones are not, and the theory points toward anatomy as the foundational differentiator. A high-resolution understanding of where the arteries are positioned drives the cautious injector toward greater precision since many practitioners will demonstrate much lower resolution mental images of the underlying vascular anatomy despite knowing all the correct anatomical terminology.
The time spent understanding subtle anatomical detail and then using that knowledge to inform your injection technique appears to be what actually cuts your vascular occlusion risk by over 70% over five years. The last thing that should go through your mind as the bevel of your needle touches the skin on your patient’s lip is the anatomy, particularly the mental image of where the arteries lie in three-dimensional space relative to your planned injection site.
Examining the anatomy through layer-based understanding
Understanding lip anatomy as injectors requires thinking in terms of layers and being able to place structures relative to each other in your mind’s eye with precision that accounts for depth, lateral position, and the potential for anatomical variation between patients. At the superficial level we encounter the dermis, followed by a layer of hypodermic fat, then the orbicularis oris muscle, and beneath that the submucosa with the mucosal layer forming the lip envelope as the deepest structure we typically consider during injection planning.
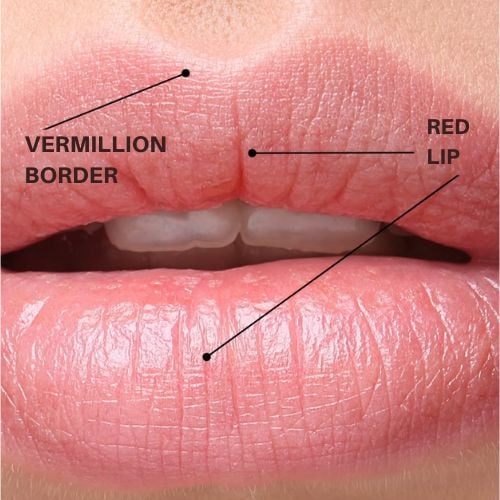
The muscle insertion into the vermilion border creates a crucial landmark that represents the divide between mucosa and dermis, providing an exceptionally useful reference point for estimating the likely position of the artery because it’s clearly visible for all practitioners during the injection process. Professor Cotofana’s research represents some of the best published work on this anatomical area, with one particularly valuable paper explaining the common depths and relative positions of the labial arteries and the likelihood of these vessels changing planes as they traverse across the lips.
This research studied 193 cadavers which constitutes a very substantial sample size by aesthetic medicine standards, with dissection performed at three different points along both the superior and inferior aspects of the lip to identify arterial position relative to the muscle. The researchers established that there are three layers where we might encounter the artery, including sandwiched between the oral mucosa and the muscle, positioned within the muscle itself, or located above the muscle in the hypodermis.
Analyzing the distribution of arterial positions
The cadaver study findings indicated that 78% of arteries were posterior to the orbicularis oris muscle, 17% were positioned intramuscularly, and 2% were located in the hypodermis, while approximately 30% of the specimens showed vessels actually crossing into different layers within the same individual. The research also reported that the superior labial artery tends to run exactly where many injection techniques place filler at the level of the vermilion border, whereas the inferior labial artery was found to be inferior to the vermilion border which works more favorably for injector safety.

One limitation of cadaver studies centers on the fact that cadavers do not represent our typical patient cohort since we primarily treat younger females in aesthetic clinics while most cadaver specimens come from very old individuals who have experienced significant volume loss over time. The depth of the artery likely differs significantly as we lose facial volume with aging, which could account for some of the discrepancies found across different published studies attempting to map labial artery position.
An ultrasound study also from Professor Cotofana examined a much younger cohort with an average age of 26 years and found the depth of the artery to be 5.6 millimeters on average from the surface of the skin, representing measurements more relevant to the patient population most practitioners actually treat. This ultrasound research discovered a different distribution of arterial positions, with approximately 58% showing the artery in the submucosal plane, 36% with intramuscular positioning, and 5% presenting with arteries in the dermis.
The most significant difference involves this paper describing the artery as running in the red lip as opposed to the vermilion border, which initially appears contradictory when we seek consistency across published anatomical research.
Resolving the apparent contradictions through dimensional thinking
The challenge with anatomical descriptions stems from our tendency to describe structures in two dimensions by default since it’s quite complex to reference alternative points of view while describing a lip from one specific perspective. When one paper describes the labial arteries as being in the vermilion border while another places them in the red lip, this represents significantly different information for an injector with high-resolution anatomical understanding.
The resolution to this apparent contradiction came while observing a tomato cut in half, which reminded me of lip cross-sections and helped explain why cadaver and ultrasound studies might describe the artery differently. As you rotate a tomato and observe how the position of a seed on its outer perimeter appears to change when viewed from the front compared to other angles, it becomes clear that perspective dramatically affects how we perceive anatomical position in two-dimensional descriptions.
In the ultrasound study examining young patients with more volume in their lips and potentially greater outward curl of the orbicularis oris muscle, the artery lies deep within the tissue, and as the lip ages the muscle insertion at the vermilion border falls relatively to the artery while the vessel itself becomes more superficial as volume is lost. This means the artery is more likely to appear parallel with the vermilion border in an older patient and positioned slightly inferior to the border but deeper in a younger patient, though the artery is rarely actually positioned in the vermilion border itself despite appearing parallel with the border from certain perspectives.
Understanding the practical implications for injection safety
The distinction between the artery being parallel to versus positioned in the vermilion border fundamentally changes what you picture when planning your injection approach. If you consider each anatomical plane on its own, it becomes reasonable to say that any injection placed in the vermilion border is always close to the artery in the horizontal dimension since the artery runs parallel to this structure, but in terms of depth the artery is almost certainly positioned significantly deeper by at least five millimeters in a younger patient with good lip volume.
Our main defense against vascular injury causing bruising and vascular occlusion therefore relies on maintaining appropriate relative depth compared to the border, and experienced injectors appear better able to discern the difference between two millimeters deep and three millimeters deep even though this represents a tiny measurement requiring substantial practice to consistently achieve. If there’s one dimension that practitioners should master as an injector, it’s depth control down to the millimeter level, and this becomes increasingly important when you consider the lips from different anatomical dimensions simultaneously.
The more lateral you position your injection in the top lip and the more medial you work on the bottom lip combined with proximity to the vermilion border, the more critical depth precision becomes for avoiding vascular complications.
Building instinctual depth awareness through deliberate practice
Every millimeter counts when you’re injecting lips, making it essential to take an extra second during each treatment to really picture in your mind’s eye exactly how many millimeters deep you’re positioned as you perform your depth check on the needle. Counting deliberately as you advance your needle to one millimeter, two millimeters, three millimeters and recognizing you better not reach five millimeters depth without strong justification helps build the instinctual awareness that makes practitioners safer as years of experience accumulate.
The more you think carefully about depth measurement during actual treatments, the more instinctual this skill becomes and the safer an injector you’ll develop into as time progresses, ultimately contributing to that 70% reduction in vascular occlusion risk that research demonstrates experienced practitioners achieve after five years of focused practice. Vascular occlusion remains the most feared complication in lip treatments precisely because the consequences can be so severe when arterial compromise occurs, making every effort to understand labial artery anatomy in three dimensions an investment in patient safety that pays dividends across your entire career in aesthetic medicine.

Dr Tim Pearce eLearning
Dr Tim Pearce MBChB BSc (Hons) MRCGP founded his eLearning concept in 2016 in order to provide readily accessible BOTOX® and dermal filler online courses for fellow Medical Aesthetics practitioners. His objective was to raise standards within the industry – a principle which remains just as relevant today.
Our exclusive video-led courses are designed to build confidence, knowledge and technique at every stage, working from foundation level to advanced treatments and management of complications.
Thousands of delegates have benefited from the courses and we’re highly rated on Trustpilot. For more information or to discuss which course is right for you, please get in touch with our friendly team.





