You may be interested


Bright Light, Better Mood: The Role of Light Therapy in Perinatal and Nonseasonal Depression
March 19, 2026


 Dr Tim Pearce
Dr Tim Pearce
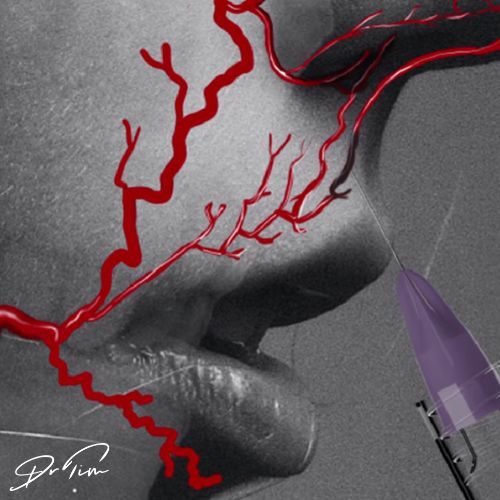
The superior labial artery refuses to follow a single rule. Published anatomy papers describe its location as routinely in or slightly above the vermilion border, but the relationship to the orbicularis oris muscle varies considerably: 60% beneath the muscle, 35% within it, and 5% above. The position can even shift within the same patient along the artery’s path.
The caliber persistent artery anomaly
Anomalous versions of this artery exist. Julie Horn (often considered the #1 lip injector in the world), recently shared an amazing video of an artery pulsating near the wet-dry border, which turns out to be a known anomaly discovered back in the seventies called a caliber persistent artery. This occurs in around 2-3% of people, Julie estimated roughly two in 50 patients from her clinical experience, which aligns with published data showing 3% prevalence.
This anomaly is interesting but remains an exception. The normal position of the artery doesn’t sit at the wet-dry border, but it can. This reality reflects what we all face each time we inject: anatomical variations exist, but we’re discussing the average arterial position that guides clinical decision-making.
The cross-sectional view that changes everything
Look at a histological specimen cut directly lengthways across the lip. This cross-section represents the most important anatomical image you’ll see because it shows where the artery tends to lie. The muscle runs down the middle of the lip, with a little hypodermic fat anterior to it, then the dermis. On the other side, underneath the muscle, sits where the artery usually positions itself.
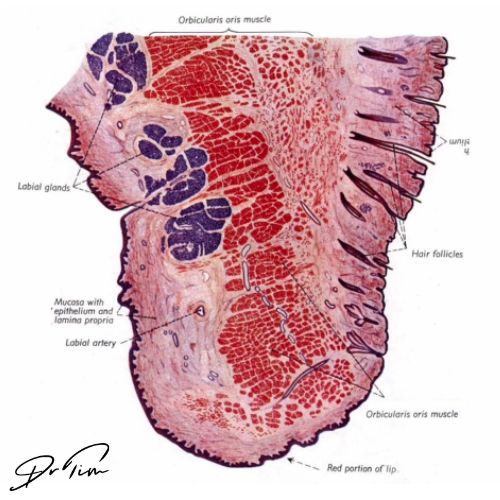
The artery doesn’t always occupy that exact point, but it usually lies just inferior to the orbicularis oris muscle. Picture where your injection goes, it’s on that anterior surface in most cases. Whether you’re using horizontal or vertical technique, it should target the anterior aspect of the lip.
The chin vessels that demand respect
When treating the chin, you’re dealing with really only two vessels likely to be hit directly: the mental artery and the submental artery. The inferior labial artery sits very nearby, but thinking purely about the chin, it should be one of those two vessels. For chin augmentation specifically, the submental artery matters more.
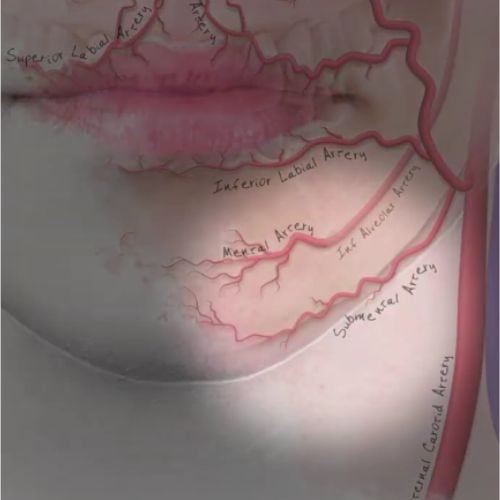
This artery comes from underneath the mandible, as the name suggests. The submental artery curves round, then supplies the anterior part of the chin. The reality is considerably more complex than the simple diagrams found in textbooks.
The submental artery supplies very important structures in the neck. The artery passes from the anterior part of the chin towards the neck, and just superior to it lie the muscles that stabilize the floor of the mouth during swallowing: the digastric muscle, geniohyoid muscle, mylohyoid muscle, and stylohyoid muscle can all be affected.
In theory, some people have a connection and anastomosis between the sublingual artery and the submental artery. This becomes extremely important because when injecting with high volumes (as we do when treating the chin), you could theoretically affect the tongue’s blood supply. This probably represents one of the worst injuries because a necrotic tongue is extremely debilitating.
The complex anatomy possible around this area deserves consideration beyond the simplified versions presented in textbooks.
Why treatment design demands anatomical understanding
What comes next in creating a treatment design? The anatomy and physiology of the face, naturally. Two elements make up this foundation: the anatomy itself, what layers and structures are you actually injecting into, and how that will change how your product behaves over time, and the physiological function those structures serve.
If this were just shape or sculpture, like working with clay where everything consists of one material, you could focus solely on aesthetics. We’re not doing that. We’re injecting a moving structure that has function, and we don’t want to upset that function while achieving good aesthetic results.
You need to think about anatomy in dynamic form. This represents one of the early mistakes people make, thinking about before and after photographs without considering facial dynamics. The point of your face, its purpose, is to communicate. That’s why facial anatomy differs from muscles elsewhere in your body.
Look at muscles in any other part of your body. Effectively they run from bone to bone, moving bones and basically moving the organism around. The difference with your face is that muscles run from bone to the surface of the skin. Their only purpose is moving the skin so we can communicate non-verbally with each other, which is a survival skill. If you cannot communicate effectively with your tribe, you’re at a huge disadvantage.
Remembering that aesthetics aren’t just static but also dynamic is essential to the skill. We need to control dynamic beauty, not just the static beauty that many people focus on in photographs.
These are rules, ratios, and functions of the face that come from understanding anatomy. This understanding comes not just from knowing the muscles and arteries, but actually knowing the depths, positions, and movement of those structures so you can create treatment designs that fit around risk (the complications side of things) while only affecting movement positively. You want to harmonize movement that may be unattractive and certainly avoid stopping movement needed for positive communication.
You need to know all the anatomical structures, and all of them are relevant: ligaments, connective tissues, SMAS, muscle, fat, deep fat pads, and superficial fat pads. The structures we’re terrified of injuring, blood vessels (arteries in particular), but also veins, nerves, and glands, all require designing treatments around them to minimize risk.
The layout of lower face muscles
Interesting differences exist with muscles in the lower face compared with other muscles in your body. Think about what the average muscle does: it connects bone to bone. Most other muscles, when they contract, have an insertion and origin point that tends to be bone to bone.
What differs about the face in particular is having many muscles connected either to other muscles or into the skin, because so much movement is required. That depends on which part you look at. I’m talking mainly about the anterior face. The anterior face includes all those muscles that control the mouth, elevate the lip, and move the chin, all skin-to-bone or bone-to-skin depending on how you’re looking at it.
The muscles of mastication are different. They are the classic bone-to-bone connections, and you don’t see those connections in the surface of the skin. When we covered the fat pads (in another video worth checking out), this explains the interesting layout where the muscle and fat pads are like tiles on a roof where they’re stacked together, and the deep fat pads actually sit on top of other muscles.
That’s the first thing that differs about muscles in the face, they don’t have the classic connections that the rest of skeletal muscle does. Next, think about how they’re actually supporting and holding structures. I kind of think about much of the midface as basically hanging off the zygoma and the maxilla. All those bony attachments are either on the maxilla or the zygoma, and they’re hanging the mouth, the nose, and the chin, all supported on those muscles anteriorly. I almost imagine it sort of hanging there, supporting. There are obviously elevators and depressors, which we’ll look at in detail.
The ligament distribution pattern
It’s important first not to get too focused on individual ligaments, but to picture the ligament distribution because that helps your understanding considerably. If you actually look at ligament distribution, most fall on an angle between the lateral and anterior face.
This change in facial function gets overlaid by anatomy. As you move from being focused more on communication to focused more on mastication, that’s where the line of ligaments sits, so they’re almost forming that boundary. If you have a look at this line of ligaments, it starts with the superior temple septum. You then have the orbicularis oculi retaining ligament, and in particular the lateral orbital thickening, which falls on this line. You have the zygomatic cutaneous ligament, by far the strongest aspect sits right on the angle of the zygoma on this line.
Following underneath that, along the masseter, you have the upper masseteric cutaneous ligaments and then the mandibular septum beneath that, and onwards finally to meet with the mandibular cutaneous ligament. This is the line of ligaments that holds the anterior face in place.
The platysmal bands consideration
This is a very superficial muscle. It’s like a sheet, but then it collects into bands, and essentially you can relax it. It’s connected into the SMAS, so if you relax it, sometimes you see jawline improvement, which can really make a good difference. That’s why it’s called the Nefertiti lift when you do toxin treatment, you create that Nefertiti-type jawline in a percentage of people.
Side effects, similarly to treating the lower face, include occasional asymmetry in the lower mouth that I’ve seen a few people get. This happens because the muscle isn’t actually as neat as it appears in a textbook, and it’s often woven into those depressors. You can sometimes see depressor anguli oris and the platysmal band kind of woven together. So occasionally people get asymmetry when they smile. I think it’s when you’re injecting very high up, but it’s worth knowing about.
Watch the full Aesthetics Mastery Show
Top 6 Aesthetics Anatomy Lessons
See the full show, which compiles Dr Tim’s top 6 anatomy lessons. Including lips, chin, platysmal bands, ligaments, and the lower face.
You can also subscribe to our YouTube channel for really useful regular tips and advice. ![]()

Dr Tim Pearce eLearning
Dr Tim Pearce MBChB BSc (Hons) MRCGP founded his eLearning concept in 2016 in order to provide readily accessible BOTOX® and dermal filler online courses for fellow Medical Aesthetics practitioners. His objective was to raise standards within the industry – a principle which remains just as relevant today.
Our exclusive video-led courses are designed to build confidence, knowledge and technique at every stage, working from foundation level to advanced treatments and management of complications.
Thousands of delegates have benefited from the courses and we’re highly rated on Trustpilot. For more information or to discuss which course is right for you, please get in touch with our friendly team.
Dermal Filler & Lips eLearning Courses
If you want to increase your knowledge about safe and effective lip filler injectable treatments, Dr Tim Pearce offers a series of fabulous courses, from foundation and upwards:
- 8D Lip Design
- Elective Lip Reversal
- Dermal Fillers Foundation Course
- Dermal Filler Complications Mastery
In addition, browse our FREE downloadable resources.




