You may be interested




 Dr Tim Pearce
Dr Tim Pearce

The techniques that make 25-year-old lips look stunning, simply don’t apply the same way to older patients. Lips change dramatically with age, and as you try to address multiple layered problems simultaneously, the complexity becomes challenging.
The difference requires a completely different consultation approach.
Three simultaneous diagnoses
Every lip consultation involves three distinct assessments happening at once: the patient’s psychology, the aesthetics troubling them in the mirror, and the underlying anatomy driving both. Breaking these down properly transforms your treatment design from guesswork into strategy.
The defensive mindset
Older patients typically approach aging from a defensive position. They’re seeking certainty and restoration, they want to return to who they were, not transform into someone new. Talk about “adding volume” or “enhancement” and you’ll watch them tense up, afraid of looking done, afraid of what their friends might say. Some of my clients describe this fear as “mutton dressed as lamb”, they desperately want to avoid drawing attention by appearing to chase youth.
This defensive psychology creates a dangerous trap. Patients request the wrong treatment out of fear, saying “don’t treat my lips” while pointing at upper lip lines. If you only address the lines without treating the lip body, you create the Homer Simpson look, that simian appearance where isolated treatment paradoxically makes them look more treated, not less.
The solution lives in education. A thorough consultation that explains lip aesthetics and demonstrates how your conservative approach protects them from the trout pout they fear will typically win them over. They need to understand that treating the lip body with small volumes actually achieves the natural restoration they’re seeking.
Emotional triggers in aging lips
The aesthetic changes in aging lips trigger specific negative emotions when patients look in the mirror. The anger element comes from lips that appear smaller relative to the face while developing lines that create a pursed, negative expression. The sadness factor stems from a downturned mouth, where lost volume underneath allows the depressor anguli oris to pull the oral commissures downward while gel fat rests on top.
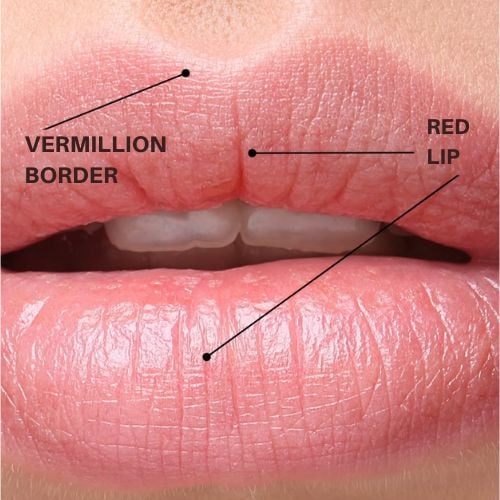
Beyond these primary emotional drivers, patients lose defining details. The vermilion border, cupid’s bow, and lower lip angles all soften and disappear as collagen breaks down and supporting structures weaken. Color and contrast fade, though redness does return temporarily after injection through increased blood flow to the area.
At the extreme end, lips become involuted. The top lip rotates inward so the white lip becomes dominant, and occasionally the lower lip prolapses outward while the upper lip involutes in. These structural changes sometimes respond to injectable treatment, but they require understanding before you can design an effective approach.
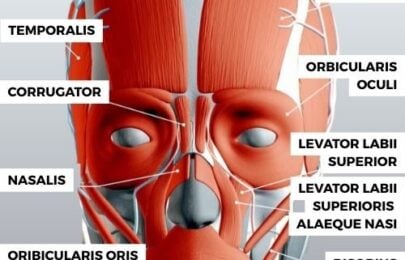
Anatomical drivers
Volume loss begins in the early 30s as the primary anatomical change. Following closely behind comes decreased integrity, reduced collagen and in some cases hypertrophic skin that creates a distinct aging pattern. Spotting which type of skin change you’re dealing with determines what treatments will actually work.
Volume changes elsewhere impact the mouth significantly. Lost volume underneath the lip combines with teeth and bone loss when patients lose teeth, all contributing to lip involution. Fat pad loss creates hypermobility, that excessively mobile mouth with pronounced pursing that happens when fat no longer resists the muscles. Muscles dominate the face when fat pads disappear, causing dramatically more lines than appropriately cushioned tissue would allow.
The glycation problem
The number one pitfall when treating upper lip lines is glycation. Practitioners struggling on forums with patients who won’t respond to treatment almost always have glycation in front of them without recognizing it.
Advanced glycation end products accumulate due to excessive blood sugar levels and react with skin macromolecules. Sun exposure accelerates the process, leading to lost protein function, impaired elasticity in tissues, blood vessels, skin, and tendons. The macromolecules become brittle and fragment easily, creating a characteristic cobblestone appearance, little islands of skin separated by crevices.
These crevices are not wrinkles. Filling them with dermal filler produces deeply unsatisfying results.
The glycation examination
Proper examination requires gloves and tactile assessment. Sit your patient down and try pulling the lines apart. Lines that separate well will unfold cleanly, revealing a crease the same color as surrounding skin, this signals you can improve the area with volume underneath.
The warning sign appears when you see crevices with a base that’s pale or pink rather than matching the rest of the skin. You’ll sense hypertrophied skin elements next to these cracks rather than simple folds. This is not a true wrinkle. These patients need skin resurfacing such as CO2 laser, not injectable treatment.
Treatment structure and zones
Technical perfection isn’t necessary to make patients happy, that’s always the primary goal. But from a pure technical perspective, more aggressive and holistic treatments do achieve superior results, so you need to consider both approaches.
Start by assessing overall mouth structure. Look for downturns or negative shapes, examining the chin, jowls, and resting lip position. These indicators point to fat pads that are either depleted or hypertrophied, which could benefit from support or reinflation depending on whether they’re resting from the side or lacking internal volume. This is where lip treatment often expands into full face treatment, which happens regularly when you consult well.
For lip-focused restoration, three zones matter:
- Structure comes first. The vermilion border, curves, and shapes define what you’d draw if sketching a lip. Assess the overall shape, check for downturns, verify important details remain visible. Structure typically gets corrected before anything else.
- Volume follows. Curvatures, projections, and relative proportions relate primarily to volume, and these usually require different injection techniques than structural corrections.
- Lines and wrinkles come last, where most practitioners mistakenly begin. Once you’ve established structure and volume, treating lines becomes dramatically easier and you avoid disproportionate results from focusing on superficial lines that then require volume adjustments that alter lip shape unpredictably.
Three injection zones
- The lip body is the main treatment area in younger patients where you’re adding volume. Include the vermilion border here as a defining point you’d treat alongside the body itself.
- The retro orbicularis oris fat pad depletes with age and isn’t commonly treated, but its loss explains why some patients develop severe lines even at rest. When you’ve lost so much volume that the orbicularis oris muscle dominates, it creates persistent lines while the patient sits doing nothing. You can address this underlying fat pad depletion.
- The hypodermic fats above the muscle represent where the visible lines actually exist, making this another common treatment zone for lip restoration.
Treating just one zone to completion creates problems. If you eliminate all top lip lines by treating only the hypodermic fat, you’ll likely cause disharmony unless you’re extremely conservative, though some patients do respond well to minimal intervention and feel satisfied with small improvements.
Treating all three zones without addressing the rest of the face creates the opposite problem: a perfectly restored mouth that doesn’t match the facial context around it. If you’re not treating holistically, you must work with smaller volumes and accept more modest results, because the more perfect you make the mouth, the more it stands out as having different volume levels than the integrated facial structure surrounding it.
Technical execution
For patients with significant fat loss underneath the orbicularis oris muscle, you can replace that volume using a cannula for safety since arteries tend to run beneath the muscle. Enter through the philtrum or at the modiolus and slide underneath, painting a thin layer of product. Feel from the inside to ensure smoothness, working slowly with small passes and minimal volume while testing their movement to observe how the product resists skin motion.
The lip body is vital for natural results in older patients with very small lips, yet this is the component they often resist because they fear looking done. A good consultation typically wins them over. Small volumes that restore slight roundness and show a hint of pink can satisfy them considerably. You’re reversing the aging process that causes inward lip rotation, so you’re rotating it slightly outward instead.
For line treatment, a cannula works well when lines are severe and you’re replacing hypodermis volume, as this is a painful, bruise-prone area where multiple needle entries would be problematic. I’ve moved toward using soft products like Juvederm Volbella, painting thin layers within the hypodermis above the muscle to soften lines before addressing deeper ones with dermal needle injections.
This creates a solid platform for the final stage: very superficial injections to restore the lines themselves. You’re working in the mid dermis with tiny micro boluses, 0.0025ml amounts where the needle barely moves. You’re watching for the line to slightly unfold, then moving to place two or three micro boluses within each line. The volumes stay extremely low to avoid structural changes, using products appropriate for superficial placement.
Psychology determines success
Not every older client needs perfection. A step in the right direction can deliver the satisfaction they’re seeking, and psychology matters more than technical achievement. You don’t need to subject patients to extensive procedures to achieve the best technical result when many (particularly those in their 80s and 90s) will be thrilled just to see a little pink and be able to apply lipstick again.
Build treatments around patient psychology and what will genuinely make them happy for the least risk. Most older patients don’t expect miracles, they’re not a difficult cohort to understand. Make sure they know what difference they’ll actually see. I show patients in the mirror while examining their lips to test line responses, and I’m completely blunt if I don’t think we’ll achieve a good result. “It’s going to be a small difference, probably visible but not dramatic. Is that still worth it to you?”
Many older patients with lips needing restoration actually need skin resurfacing rather than injectables. Some need surgical lifting as part of a facelift. We’re always trying to recommend the right solution for their happiness, which isn’t necessarily always about technical results as much as what fits their circumstances, their budget, their attitude toward surgery, their attitude toward lasers and injectables, and what they actually want to achieve within the remit of available treatments.
If you’ve only ever done conservative half-milliliter treatments focused just on lines, implement these broader approaches in small steps. Start with modest volumes, choose laid-back patients who don’t mind taking a slower journey with you, and build your confidence gradually. Don’t bite off more than you can chew.

Dr Tim Pearce eLearning
Dr Tim Pearce MBChB BSc (Hons) MRCGP founded his eLearning concept in 2016 in order to provide readily accessible BOTOX® and dermal filler online courses for fellow Medical Aesthetics practitioners. His objective was to raise standards within the industry – a principle which remains just as relevant today.
Our exclusive video-led courses are designed to build confidence, knowledge and technique at every stage, working from foundation level to advanced treatments and management of complications.
Thousands of delegates have benefited from the courses and we’re highly rated on Trustpilot. For more information or to discuss which course is right for you, please get in touch with our friendly team.
Dermal Filler & Lips eLearning Courses
If you want to increase your knowledge about safe and effective lip filler injectable treatments, Dr Tim Pearce offers a series of fabulous courses, from foundation and upwards:
- 8D Lip Design
- Elective Lip Reversal
- Dermal Fillers Foundation Course
- Dermal Filler Complications Mastery
In addition, browse our FREE downloadable resources.