FREE Complications Webinar
Want to overcome your fear of complications and confidently master anatomy?
Join us for one of Dr Tim's FREE upcoming webinars. .
Check dates here and save your spot
 Dr Tim Pearce
Dr Tim Pearce
Picture this: You’ve just injected what looks like a perfectly defined jawline, but when your patient turns their head, suddenly they look wider and longer, tilting toward a more masculine appearance than they should. The problem isn’t your technique, it’s that you’ve been staring at one side of their face the entire time.
The jawline sits at the intersection of multiple facial planes, which means every needle placement changes how the chin meets the jaw, how the jaw meets the neck, how all of it looks when your patient walks out the door and sees themselves in natural lighting from every angle. You can’t adjust one plane without affecting the others, which creates what might be the hardest part of treating jawlines: you need three-dimensional awareness while injecting.
Look across your patient like this the whole time, moving around them instead of planting yourself on one side and working through your technique like you’re checking boxes. Otherwise you’ll end up with a beautiful definition that photographs well from exactly one angle, which helps nobody.
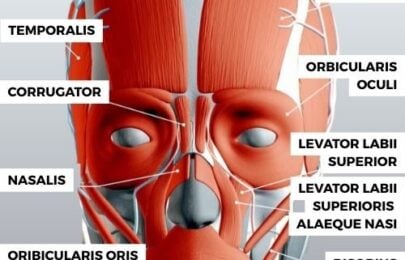
Two vessels dominate your risk assessment here: the submental artery and the facial artery. The submental artery runs on the anterior part of the mandible, typically not quite on the bone but it can be, typically not on the midline but it can be (more common in females, from what I’ve seen). The facial artery emerges in front of the masseter muscle and curls up heading towards the alar base where it becomes the angular artery.
First thing when I’m treating a jawline is to feel for the notch in the jaw, which tells you where the facial artery sits. If you’re using ultrasound, scan around the chin to see where those vessels are, because this helps you choose the right instrument, cannula or needle, and place it where the vessel isn’t.
The parotid gland sits inferior to the zygoma on top of the masseter muscle, running down underneath it like this. The mental artery exists but it’s small, not really a place where we tend to put needles often, and if you’re using a cannula it’s probably small enough and easy enough to move out of the way to not be high risk.
Here’s where practitioners get into trouble: they treat male and female jawlines the same way, when the goals are fundamentally different.
For females, the goal is a jawline less dominant than the cheeks, petite chins terminating in the midpoint, narrower gonial angle so the cheeks dominate over the jawline, relatively narrow and pointed downward to create a heart-shaped face. In females, it’s very easy to tilt them into looking masculine by making them wider at any point. You can make them wider at the chin or jawline or gonial angle, all of those when they tilt too far become masculinizing.
Men are easier because they just need to be bigger and more dominant, which means you can add product that creates shape and not worry so much about overtreatment. Making them wider at the chin is less of a critical error than in a female.
Many chins can break the facial plane, which usually runs from the nasion down towards the chin. You’ll see diagrams where the chin is flush with the nasion, but look at really good-looking people and often the chin is a little bit stronger than that.

Take Margot Robbie’s side profile, I found a picture described as “the profile of a goddess” and it clearly breaks the facial plane, so I’m not afraid of over projection a little bit according to that rule. What I am definitely afraid of is inferior projection in a female, making them look masculine through the lateral and inferior aspects, which are most commonly overtreated.
Sometimes you just get a little bump where the under part of the chin has been overtreated and it doesn’t quite fit into the jawline, which probably leads to one of the hardest parts of doing the jawline: it’s actually the meeting point of multiple facial planes, so you can’t adjust one without affecting the other.
If you’re treating a female, start with the gonial angle but remember not to make it too straight, because a completely straight jawline in a female looks like an adolescent boy. It’s edgy, a lot of beauty is edgy, but it can easily tip into just looking gaunt or masculine, so a little bit in the gonial angle becomes my main injection point laterally.

Then the chin, where in females we tend to have a central injection point while in men you have two injection points either side. The actual injection point changes according to whether I want to project anteriorly, inferiorly, or a mix of both (which is very common). In fact, the most common way I inject chins in females is so that the path of the needle reflects the path of the jawline, as if the chin is being continued rather than the front of the chin just being added on.
I’m trying to change all three planes simultaneously rather than treat one, correct it, then inject somewhere else, which means the injection point varies according to where I’m intending the projection to go, lateral, anterior, inferior, or a mix of all.
A patient posted online about her jaw filler experience after getting what’s called Radiesse, a non-dissolvable filler. The injector told her it would make her face more slim looking and chiseled, but here’s what actually happened: the pictures that you see online of jawlines that look perfectly straight are always shot from the side angle, because many people do this unconsciously in pictures when they take a selfie, it makes your jawline look better.
The problem with this approach is that the clinician made a defined jawline but only from one angle, so as soon as the face rotates to look straight at you, you end up with this bulkiness. From the side it creates a lovely shadow and looks better, but our faces are three-dimensional and most of the time we’re looking at people head-on.
She felt a downgrade in her appearance overall from this treatment because she had high cheekbones that didn’t match the protrusion of her new jawline, making her face look more masculine. Her left side came out way more than her right side, looking asymmetrical and horrible for 2 years, why 2 years? Because she used a non-reversible product.
We have hyaluronic acids that now last similar lengths of time and you can easily reverse them, yet the drug companies who make non-reversible products don’t like me, I’ve even had letters trying to get me to take my videos down. Good luck with that because I’m talking to a clinical audience and I don’t actually sell any treatments through my page, so I can talk about these prescription products.
I hate the idea that they’ve tried to get these things removed from my page because they don’t want the negative press, when patients need to know the risks of non-reversible products. They’re not saying they’re not right for someone, but they’re not right for the average person, surely you want the option of reversibility.
This patient had to have a downgrade in her self-esteem and confidence for 2 years because of a product that couldn’t be dealt with appropriately, which is exactly why reversibility matters so much in a treatment area as complex as the jawline.
When you see me do jawlines, I’m often looking across the patient like this the whole time, trying to get three-dimensional awareness of what’s going on rather than treating the patient while just looking at one side. Otherwise what you end up with is beautiful definition that turns into a disaster when they turn their head and suddenly look wider and longer than they should.
Think about all the planes and inject accordingly to the feminine shape you’re trying to create in females or the more masculine shape you’re trying to create in men, because men are easier for this reason, over projection, over widening, making the chin wider is less of a critical error than in a female.
Common injection points if you’re treating a female: start with the gonial angle (not too straight), then the chin with a central injection point. For men: two injection points either side of the chin, where the injection point will change according to whether you want to project anteriorly, inferiorly, or both.
In fact, the most common way I inject chins with females is so that the path of the needle reflects the path of the jawline, as if the chin is being continued rather than the front of the chin just being added on, which means I’m trying to change all three planes simultaneously rather than just treat one and then correct it and then inject somewhere else.
The jawline is a very complex, challenging area where many clinicians initially love it during training, then hate it when they get back to their clinics because of the variety of different jawlines we’re challenged to treat. The key is understanding the anatomy, knowing where those vessels are, choosing your patients carefully, and never, ever injecting while staring at just one side of their face.
Join us for one of Dr Tim's FREE upcoming webinars. .
Check dates here and save your spot

Dr Tim Pearce MBChB BSc (Hons) MRCGP founded his eLearning concept in 2016 in order to provide readily accessible BOTOX® and dermal filler online courses for fellow Medical Aesthetics practitioners. His objective was to raise standards within the industry – a principle which remains just as relevant today.
Our exclusive video-led courses are designed to build confidence, knowledge and technique at every stage, working from foundation level to advanced treatments and management of complications.
Thousands of delegates have benefited from the courses and we’re highly rated on Trustpilot. For more information or to discuss which course is right for you, please get in touch with our friendly team.