FREE Complications Webinar
Want to overcome your fear of complications and confidently master anatomy?
Join us for one of Dr Tim's FREE upcoming webinars. .
Check dates here and save your spot

March 19, 2026
 Dr Tim Pearce
Dr Tim Pearce
 Here’s something that took me years to properly internalise: the face you’re injecting is fundamentally different from every other part of the body. Not slightly different, but fundamentally. Once you grasp why, your entire approach to treatment design changes.
Here’s something that took me years to properly internalise: the face you’re injecting is fundamentally different from every other part of the body. Not slightly different, but fundamentally. Once you grasp why, your entire approach to treatment design changes.
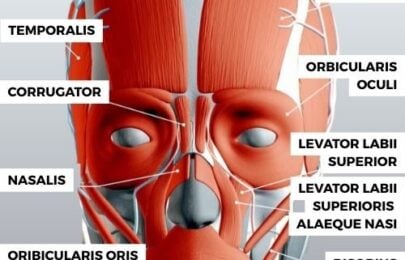
Most muscles connect bone to bone. They move the skeleton. Biceps, quadriceps, deltoids, all following that same blueprint. But facial muscles run from bone to skin. Their job isn’t locomotion, it’s communication – moving the skin surface so you can signal fear, joy, suspicion, attraction to the people around you without saying a word.
This distinction matters because we’re not sculpting clay, we’re injecting a moving, communicating structure. The aesthetic result in a photograph is one thing. The aesthetic result when your patient laughs, frowns, or raises an eyebrow, is something else entirely.

Where exactly is the superior labial artery when you push your needle into the lip?
Clinical papers describe it running above or within the vermilion border. But its relationship to the orbicularis oris muscle follows a more useful pattern: 60% of the time it sits beneath the muscle, 35% within the muscle itself, and about 5% above. That variability can occur in the same patient, the vessel wiggles around along its course.
Picture a histological cross-section. The orbicularis oris runs down the centre, with hypodermic fat anterior to it, then dermis. Posterior to the muscle, that’s where the artery typically lives. Your injection lands on that anterior surface whether you approach horizontally or vertically. Stay superficial, and you’re progressively moving away from where the vessel usually sits.
Julie Horne shared a video showing an artery visibly pulsating near the wet-dry border – not where you’d expect it and not deep. It was right there at the surface.
This is a caliber persistent artery, an anomaly first documented in the 1970s, present in roughly 2-3% of patients. Julie estimates she sees it in about two out of every fifty patients, which aligns with the published data. The vessel penetrates the submucosa without losing diameter, ending up much more superficial than normal anatomy would suggest.
Practically, this means the normal position of the labial artery isn’t at the wet-dry border. But it can be, and that’s the tension we navigate with every injection, probability versus possibility. The statistics suggest one thing; the patient in front of you might be the exception.

Two vessels matter in chin augmentation: the mental artery and the submental artery. For most procedures, particularly lower chin work, the submental artery is the one to respect.
It curves underneath the mandible, then supplies the anterior chin. Simple enough on a diagram. But those simplified textbook illustrations miss the structures this vessel feeds: the digastric, geniohyoid, mylohyoid, and stylohyoid muscles, all involved in stabilising the floor of your mouth when you swallow.
This is why patients with chin vascular complications sometimes report pain during swallowing. The ischemia affects muscles they didn’t know they had.
And then there’s the worst-case scenario. In some patients, an anastomosis exists between the sublingual artery and the submental artery. Chin augmentation typically involves high volumes. If that filler compromises the submental artery in a patient with this connection, you’re potentially affecting blood supply to the tongue. A necrotic tongue is one of the most debilitating injuries in aesthetic medicine, extremely difficult to manage, life-altering for the patient.
None of this means you shouldn’t augment chins. It means you should understand what you’re actually working around.
I think of the anterior midface as hanging off the zygoma and maxilla. Those bony attachments support everything below, mouth, nose, chin, like scaffolding holding a structure in place.
The muscles of mastication work differently. They follow the traditional bone-to-bone pattern, which is why chewing doesn’t visibly move your skin surface the way smiling does. The anterior face and the lateral face have distinct functions, distinct anatomy.
When you start viewing fat pads and muscles as layered like tiles on a roof, stacking together, deep fat pads sitting on underlying muscles, the behaviour of injected product starts making more sense. Why does something migrate here but not there? Why does a treatment hold in one patient and shifts in another?
Memorising ligaments one by one is the hard way. Understanding their distribution pattern is the shortcut that actually works.
Most facial ligaments fall along an angle between the lateral and anterior face. This line marks where communication anatomy transitions to mastication anatomy, a functional boundary overlaid on the structure.
Follow it: superior temporal septum, then the orbicularis oculi retaining ligament with its lateral orbital thickening, then the zygomatic cutaneous ligament at the angle of the zygoma (the strongest point on this line), then the upper masseteric cutaneous ligaments along the masseter, the mandibular septum below that, and finally the mandibular cutaneous ligament. One continuous system holding the anterior face where it belongs.
Once you see it as a line rather than a list, the anatomy clicks.
The platysma is a superficial sheet that collects into those vertical bands on the neck. Relax it with toxin, and in some patients you’ll see genuine improvement in jawline definition, the Nefertiti lift effect, named for that Egyptian queen’s famously elegant neck.
But the platysma doesn’t respect textbook boundaries.
The muscle fibres weave into the depressor anguli oris. Sometimes you can actually see where they’re connected. Inject high on the neck, and occasionally patients develop asymmetry when they smile, the mouth pulling differently on one side. It’s temporary, but it catches practitioners off guard because the anatomy in reality is messier than the anatomy in illustrations.
The lesson applies broadly: if you’re treating the lower face or neck, expect that muscles interweave in ways the diagrams simplify.
One of the earlier mistakes most injectors make, myself included, is designing treatments around before and after photographs. You see the deflation, you add volume, you photograph again. The static result looks good.
Then the patient animates. They laugh, they frown, they raise their eyebrows in surprise. And sometimes what looked beautiful at rest becomes strange in motion.
The purpose of the face is communication. If you interrupt that, if the expressions that signal warmth or attention or interest become muted or distorted, you’ve compromised something more important than a contour line.
Effective treatment design means knowing depths, positions, how structures move. Ligaments, connective tissue, SMAS, muscles, arteries, veins, fat pads deep and superficial, nerves, glands, all of it factors in. Not because you need to recite it like an exam, but because you need to predict what your product will do in a living, moving face.
The goal isn’t avoiding injury, though that matters. The goal is harmonising movement, improving what’s unattractive while preserving the expressions your patient needs to connect with other people.
In this episode, we’ve compiled Dr Tim’s top 6 anatomy lessons. Including lips, chin, platysmal bands, ligaments, and the lower face.
You can also subscribe to our YouTube channel for really useful regular tips and advice. ![]()
Join us for one of Dr Tim's FREE upcoming webinars. .
Check dates here and save your spot

Dr Tim Pearce MBChB BSc (Hons) MRCGP founded his eLearning concept in 2016 in order to provide readily accessible BOTOX® and dermal filler online courses for fellow Medical Aesthetics practitioners. His objective was to raise standards within the industry – a principle which remains just as relevant today.
Our exclusive video-led courses are designed to build confidence, knowledge and technique at every stage, working from foundation level to advanced treatments and management of complications.
Thousands of delegates have benefited from the courses and we’re highly rated on Trustpilot. For more information or to discuss which course is right for you, please get in touch with our friendly team.