You may be interested





 Dr Tim Pearce
Dr Tim Pearce

Many aesthetic practitioners may have used Hyalase® (Hyaluronidase) for an elective reversal of a hyaluronic acid-based dermal filler treatment, but not all have had to use it in an emergency, thankfully.
The first piece of advice should this happen, and it is highly likely that it will at some point in your career, is to stay calm, do not freak out, keep your emotions in check for the sake of your patient. Keep them calm and manage their expectations that you know what you are doing, that this will take some time to resolve, but you will be there every step of the way. Ultimately, you need to be prepared for the worst.
Dr Tim Pearce, who saw his first vascular occlusion whilst in training with another practitioner, is here to discuss what you need to take into account when treating a vascular occlusion, how much Hyalase to use, how much you need to stock to be safe rather than sorry, and how to access it if you cannot hold stock.
Dr Tim will be discussing more medical aesthetic training tips as part of his upcoming webinar series, so if you’re looking to increase your CPD-certified learning and want reassurance about how you’re treating patients, then step one is to register for the free webinars by Dr Tim.
Things to consider when treating a vascular occlusion
Understanding the variables involved when dissolving dermal filler is your first step.
- Different types of filler – Hyaluronic acid (HA) based fillers can be designed and cross-linked to last for different lengths of time, sometimes upwards of 12 months, which means they will take longer to dissolve and require more hyaluronidase.
- How much filler is in there? – The size of the bolus of filler deposited will affect how significant the occlusion is and the difficulty in dissolving it.
- How long has it been since the occlusion occurred? – There is a big difference between an occlusion that has just happened, the emergency, and one which is now delayed as it is 3 days or a week old.
- Is it a full occlusion or a partial occlusion? – The amount of blood flow which is compromised.
- Temperature – Both the ambient temperature and that of the patient can influence blood flow.
- Patient’s cardiac output
- Massage – Does this help relieve the occlusion by displacing the filler?
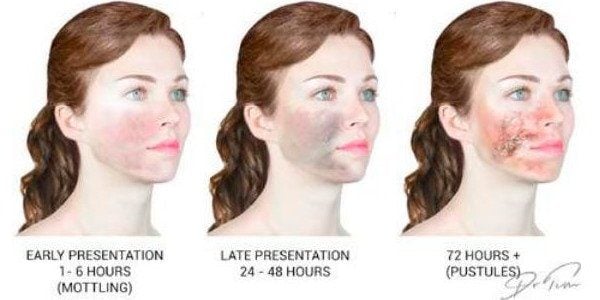
Diagnosing a vascular occlusion
There are various clues that you can look for when identifying and diagnosing a vascular occlusion.
- Area of skin is persistently pale
- Capillary refill is absent or very sluggish. Be mindful of haematoma formation which can influence capillary refill but is not necessarily an occlusion. If you would like guidance about how to tell the difference between a vascular occlusion and a haematoma, check out this YouTube show Dr Tim created on the topic.
- Initial injection triggered an arterial spasm
- Area of pallor distal to the injection site
- Pricking the skin yields no blood
- Usually the area is painful immediately and gets more painful if left untreated.
Hyalase Emergency Reversal Protocol
You first need to diagnose the situation and apply a warm compress. There is an option to run a hyaluronidase allergy test, but many do not in an emergency.
Dr Tim feels that it is important to seek help, guidance and more importantly support from another practitioner. This can be a colleague, trainer, prescriber, or mentor. This person will help you to cope, think clearly, and guide you through your training. Think of them as your co-pilot, there to help you to safely land the plane.
Take your time and deliver the Hyalase, monitoring improvement as you go. It can take upwards of an hour to resolve vascular occlusions, so be prepared to keep working at it.
As you add in a volume of hyaluronidase, it will get to work infiltrating the area and dissolving the HA. If the area starts to appear ‘empty’, yet the blood flow is still compromised, this will be a trigger for you to decide if you need to add more. It is important to maintain a concentration of Hyalase to achieve the goal, there is no magic number of vials, or a one-size-fits-all approach to the management of vascular occlusions.
Do not be tempted to send the patient home because you have used ‘x’ number of vials of hyaluronidase. Keep going until the capillary refill is restored, even if you have to source more. Rather than small doses of product every 5 minutes, Dr Tim advises frequent (every 15-20 minutes), high dosing of Hyalase to flood the area, followed by 15-20 minutes with a warm compress, and repeat.
 For more information on using hyaluronidase to manage vascular occlusions caused by dermal filler injections, we recommend downloading Dr Tim Pearce’s Emergency Reversal Protocol.
For more information on using hyaluronidase to manage vascular occlusions caused by dermal filler injections, we recommend downloading Dr Tim Pearce’s Emergency Reversal Protocol.
How many vials of Hyalase should I stock to be safe?
Dr Tim recommends carrying at least six vials of hyaluronidase in your clinic. This will vary depending on the number of clinicians injecting at the practice at any one time, to cover a worst-case scenario of multiple problems at the same.
In England, only doctors and dentists can hold stock. Nurse prescribers can only hold stock in Scotland. This barrier often means that INPs and non-prescribers get a prescription for Hyalase in their own name. Should an emergency arise, they have the defence that it was in the patient’s best interest to use the medication which was named for someone else. To the best of our knowledge this has not been tested in court.
In this case, the only lawful way to stock Hyalase would be to secure a prescription for every new patient, meaning that you have a named emergency pack for each patient at your clinic, which you renew approximately every 18 months. Most practitioners do not do this for reasons of practicality and cost. You can however choose to charge the patient for this as it can be sold as a safety and insurance provision, which can also engender patient loyalty.
Are you still anxious about delivering cosmetic injectables safely?
If you want to learn more about mastering medical aesthetic treatments and complications, or conquering the anxiety of where to place your needle, then register for the next Dr Tim webinar.
Dr Tim Pearce eLearning
Dr Tim Pearce MBChB BSc (Hons) MRCGP founded his eLearning concept in 2016 in order to provide readily accessible BOTOX® and dermal filler online courses for fellow Medical Aesthetics practitioners. His objective was to raise standards within the industry – a principle which remains just as relevant today.
Our exclusive video-led courses are designed to build confidence, knowledge and technique at every stage, working from foundation level to advanced treatments and management of complications.
Thousands of delegates have benefited from the courses and we’re highly rated on Trustpilot. For more information or to discuss which course is right for you, please get in touch with our friendly team.






Comments (4)
a huxley
Dec 01, 2020Great blog article. Really looking forward to read more. Fantastic.
Pam
Nov 29, 2020I love your writing style really enjoying this site.
sikis izle
Nov 12, 2020If you want to use the photo it would also be good to check with the artist beforehand in case it is subject to copyright. Best wishes. Aaren Reggis Sela
Ashley Scott
Nov 12, 2020Hi there, all of the images in the blog have been produced by us.
Comments are closed.